Open fittings may be a mixed blessing. On one hand, more people with a high frequency hearing loss will agree to wear hearing aids that are almost totally free of occlusion, and the fit is instant and easy. On the other hand, the indiscriminant use of open fittings can compromise the integrity of fittings, especially audibility in the important high frequencies. Because open fitting, to a large extent, is similar to the use of a vent with an extremely large diameter, this article reviews the acoustic effects of vent dimensions.
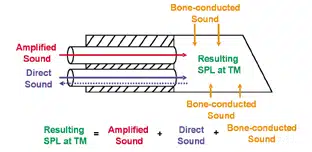
We typically consider sounds at the eardrum to be a function of the output of the hearing aid moderated by the residual volume between the tip of the hearing aid/earmold and the eardrum. To a large extent, this is true for an occluding hearing aid (one without any vents or leakage) and when the wearer listens to sounds from their environments. On the other hand, with a vented hearing aid and when the wearer talks, the overall sound pressure level at the eardrum also includes direct sounds that enter (or leave) through the vents (and any unintentional leakage) and bone-conducted sounds generated from the wearer’s voice. The contribution of each source varies depending on the state of the wearer (speaking versus listening) and the size of the leakage (or venting), in addition to the gain settings on the hearing aid. Figure 1 shows a simplified diagram of the three sources of sound.

|
| FIGURE 1. Sources of sound at the eardrum. |
In the extreme case of someone with a high frequency hearing loss who is speaking while wearing a closed earmold, the low frequency SPL at the eardrum is dominated by the bone-conducted sounds.1 In an open-fitting situation, sounds entering directly through the vent opening will have a larger contribution to the SPL at the eardrum.
Sounds Leaving the Ear
Low frequency output. The effect of venting on the acoustic output of a hearing aid is well documented. Figure 2 shows the effect of vent diameter and vent length on the output frequency response. A straight line at “0” would suggest no change to the output relative to measurement made with an occluding earmold; data above “0” suggest a gain increase (from resonance) while that below “0” suggest gain reduction with the specific vent dimension (length and diameter).

|
| FIGURE 2. Effect of vent length on low frequency output for three vent diameters (1 mm in blue, 2 mm in green, and 3 mm in red). The solid line shows the result of a 6 mm-long vent, while the dotted line shows that of a 22 mm-long vent. A straight line at “0” would suggest no change to the output measured with an occluding earmold; data above “0” suggest a gain increase (from resonance) while that below “0” suggest gain reduction with the specific vent dimension (length and diameter). |
The solid line shows the result of a 6 mm-long vent, while the dotted line shows that of a 22 mm-long vent. For both vent lengths, one sees more low-frequency gain reduction as the vent diameter increases. For example, one sees that the output at 200 Hz is reduced by 7-8 dB with a 1 mm vent diameter, but as much as 28 dB reduction with a 3 mm vent diameter. Thus, an increase in vent diameter leads to a reduction in low frequency output below 1000 Hz.
A vent is a tube. As such, it is subject to tubing resonance. Figure 2 also shows that a change in vent diameter leads to a shift in the vent-associated resonance. For the 6mm-long vent, the resonance peak occurs at around 400 Hz when the vent diameter is 1 mm. It becomes 800 Hz and 1200 Hz when the diameter is 2 mm and 3 mm, respectively. The real-ear SPL is higher than the coupler response measured at the same frequencies when a vent is used.
Figure 2 also shows the effect of vent length on the low frequency output. The longer vent (eg, 22 mm) differs from the shorter one (eg, 6 mm) in two aspects. First, the longer vent has the vent-associated resonance at a lower frequency. In this case, the resonance is at 300 Hz for the longer vent and 400 Hz for the shorter vent when both have a 1 mm vent diameter. Second, the longer vent is less effective than the shorter vent in reducing low frequency output.
In summary, as vent diameter increases, real-ear low frequency output decreases, and the frequency at which vent-associated resonance occurs increases. In contrast, as vent length increases, gain reduction in the low frequency decreases and the frequency at which vent-associated resonance occurs decreases.

|
 |
| FIGURE 3a-b. Maximum gain before feedback for the 15-channel Diva hearing aid in the BTE model (top, 3a) and ITE model (bottom, 3b). |
Maximum gain before feedback. Vent diameter also affects the real-ear high frequency output by limiting its maximum gain before feedback. Figure 3a shows the average maximum gain of a 15-channel, moderate-gain behind-the-ear (BTE) hearing aid (Diva SD-9) when different vent diameters are used; Figure 3b shows the same for an ITE hearing aid (Diva SD-X). The data were based on 10 subjects with primarily a high-frequency sensorineural hearing loss when the active feedback cancellation algorithm on the hearing aid was deactivated.
Figure 3a shows that, with a closed earmold (blue curve), as much as 60 dB of gain is available in the low frequencies but only 50 dB is available in the high frequencies. As expected, when the vent diameter increases, the available gain decreases. The decrease is more rapid in the high frequencies than in the low frequencies. Indeed, not much gain decrease is observed below 500 Hz. When the earmold is replaced with a tube fitting, only 20 dB of maximum gain before feedback is available in the 2-3 kHz region.
Maximum gain on the ITE shows a similar trend: gain decreases as vent diameter increases. However, there is less available gain in the high frequency region for the ITE than for the BTE at the same vent diameter. This is due to the closer proximity between the microphone and the receiver in the ITE than in the BTE. These values (with the active feedback cancellation off) are similar to Dillon’s measurements.2
The information on the maximum available gain before feedback has significant implications in the choice of vent diameter and our clinical practice on the use of open-fittings.
Open-fittings reduce high frequency gain. Open fittings (or larger vent diameters), for the most part, have been used for people with a high frequency hearing loss. It should be clear from the above observations that the rationale behind this practice is to maximize “comfort” with one’s own voice and not the audibility of high frequency sounds. Indeed, an open fitting typically results in poorer high frequency audibility. The clinicians and the wearers must understand the objectives (and limitations) of open-fitting so realistic expectations can be formed.

|
| FIGURE 4. Word recognition score in quiet (30 dB HL presentation level) as a function of vent diameter in the Senso Diva SD-9X ITC hearing aid. |
Compromises on speech intelligibility. The reduction in high frequency gain would limit the amount of speech cues available to hearing instrument wearers. This may affect speech intelligibility. Figure 4 shows the word recognition scores as a function of vent diameter (in a Diva SD-9X ITC) when a group of mildly sloping high frequency hearing loss subjects were tested with CASPA3 words in quiet at a 30 dBHL level. A systematic decrease in word recognition score was observed as the vent diameter was increased beyond 1 mm. Almost 20% decrease in speech recognition score was observed between a 1 mm vent diameter and the IROS vent (4.5 mm diameter). The limited available gain with the larger vent diameter may be one reason for the decrease in performance.
Advantages of active feedback cancellation. The limited gain before feedback and its effect on speech intelligibility suggests the need to be conservative in venting when speech intelligibility is the main concern. On the other hand, when it is necessary to use a large vent, such as open fitting to maximize comfort (eg, minimize occlusion), one should secure means to ensure the availability of as much gain as possible to minimize intelligibility loss.

|
| FIGURE 5. Changes in maximum available gain for different vent diameters in an ITC hearing aid. |
The use of an active feedback cancellation algorithm may be the only solution. Figure 5 shows the increase in available gain before feedback with the Diva active feedback cancellation algorithm. Different vent diameters, including an IROS vent, are used. One can see that the advantage of an active feedback algorithm is an increase in the available gain beyond 1000 Hz. The effect increases as the vent diameter increases. For example, it is only about 5 dB up to 3000 Hz with a closed earmold, compared to as much as 10 dB up to 7000 Hz in the IROS vent. The need for an active feedback cancellation algorithm in a hearing aid increases as the required vent diameter increases.
Bone-Conducted Sounds (Occlusion Effect)
Because a vent (or acoustic leakage) provides a direct link between the wearers’ acoustic environments and their ear-canals, one would expect similar vent effects on bone conducted sounds (or the occlusion effect) and the amplified sounds from a hearing aid.

|
 |
| FIGURE 6a-b. Occlusion effect for different vent diameters in a BTE (top, 6a) and ITC (bottom, 6b) Diva hearing aid. |
Objective OE ratings. Figure 6 shows the average occlusion effect as the vent diameter is changed in a BTE (Figure 6a) and in an ITC (Figure 6b) hearing aid. The OE is measured as the difference between the real-ear occluded response (REORv) and the real-ear unaided response (REURv) during vocalization of /i/. For both styles of hearing aids, the average OE has a peak frequency around 300-400 Hz with a peak amplitude of about 20 dB. On average, the OE decreases by about 4 dB for every 1 mm increase in the vent diameter. For a 3 mm vent diameter, the average OE is about 6-8 dB. Although tube fitting (in the BTE only) results in virtually no OE, the IROS vent (which has an average diameter of 4.5 mm) in the ITC still showed almost 5 dB of OE around the 400-500 Hz region.
The peak frequency of occlusion increases as the vent diameter increases. These results show that OE is a function of the vent characteristics and not a function of the hearing aid style. It suggests the possibility that the magnitude of the OE may be predictable if the vent dimensions are known.

|
| FIGURE 7. Relationship between occlusion effect (in dB) and acoustic mass (in log Henry). From Kuk et al 2005.4 |
To further explore that possibility, we plotted the acoustic mass of the vent against the measured occlusion effect for each individual subject.4 The acoustic mass is directly proportional to the length of the vent and inversely proportional to the square of the vent diameter.2 The regression lines in Figure 7 show that the objective OE is a function of the acoustic mass of the vent. The larger the acoustic mass (or the smaller vent diameter or longer vent length), the higher the OE. In other words, the OE is a physical quantity that can be estimated based on the dimensions of the vent system. The observed differences among subjects are most likely related to the individual’s middle ear characteristics and their interaction with the vent configurations.

|
| FIGURE 8. Relationship between subjective occlusion rating and vent diameters. |
Subjective OE ratings. While the objective OE is measurable and predictable from the vent dimensions, the subjective occlusion effect or occlusion rating may not be easily predicted. Figure 8 shows the individual subjective occlusion ratings (with a rating of 1 being “own voice very hollow” and 10 being “own voice very natural, no hollowness”) as a function of vent dimensions. The median ratings are connected by the solid line. No change in subjective rating is seen as the vent diameter increases from 0 mm to 1 mm. The most significant change occurs when the vent diameter increases from 1 mm to 2 mm. Further increases in vent diameters do not improve subjective occlusion ratings.
This suggests that the relationship between subjective OE and objective OE is not a simple 1-to-1 relationship. Beyond a 2 mm vent diameter, subjective OE is not likely to improve simply with a larger vent diameter (even though the objective OE is lowered). This highlights the complexity of the subjective occlusion rating and suggests that additional mechanism is necessary to yield an acceptable rating of one’s own voice.
Sounds Entering into the Ear (Direct Sounds)
One of the possible reasons for the imperfect relationship between subjective OE rating and objective OE and the decrease in word recognition score with a larger vent diameter may be related to the interaction of the amplified sounds with the direct sounds that enter through the vent. As discussed in Figure 1, the SPL at the eardrum is the result of the interactions of the amplified sounds and the direct sounds that enter through the vent. Figure 9 shows the change in SPL (or attenuation/gain) at the eardrum resulting from using inserts of different vent diameters when the reference sound is presented at the ear canal entrance. A value larger than “0” indicates that the SPL is higher at the eardrum than at the ear canal entrance reference; a number smaller than “0” suggests that the insert attenuates sounds so they are softer at the eardrum than at the entrance.

|
| FIGURE 9. Attenuation characteristics of inserts with different vent diameters. The unaided response (REUR) is also included for comparison. |
Figure 9 shows the typical ear canal resonance around 3000 Hz, suggesting that the input sound is enhanced by almost 20 dB around that frequency in an open-fitting situation. With a vented, occluding earmold, the input sounds may be increased or decreased at the eardrum depending on the vent diameter. With a completely closed earmold, the input is decreased by almost 20 dB in the high frequencies. Less attenuation is noted as the vent diameter increases. Furthermore, at a vent diameter of 3 mm, the input is enhanced by almost 3 dB across the frequencies up to 4000 Hz. It is expected that a larger vent diameter may enhance the input to a level between that provided by the open ear and the 3 mm vent conditions. This naturally enhanced sound is a main source of interaction with the directly amplified sounds.
When the natural sounds and the amplified sounds around 2000-3000 Hz are similar in magnitude and phase characteristics, they add to result in an output at the eardrum that is 3-6 dB higher than either of the input alone. On the other hand, if these two sounds are of the same magnitude but out of phase, cancellation will occur to result in a lower output and even negative gain. This phase cancellation may occur around 3000 Hz (from the ear canal resonance) and in the lower frequencies (from the vent associated resonance) when the gain provided by the hearing aid is similar in magnitude but opposite in phase to the resonant frequencies. This will result in irregular “dips” being displayed in the measured real-ear responses.
The perceptual consequence of phase cancellation is poor sound quality (rougher, harsher sound) and—depending on the frequencies where phase cancellation occurs—speech understanding may be affected. It may also be a reason why, even with an open tube fitting, subjective OE was still not a perfect “10” (discussed earlier). To further improve the sound quality of a hearing aid, these frequencies where phase cancellation will likely occur must be accounted for in the design stage in order to minimize its occurrence. (For a discussion on hearing aid design concepts and phase cancellation, see Kuk et al’s article5).
So, What’s the Optimal Vent Diameter?
As shown above, open fitting minimizes subjective and objective occlusion effects; however, it does so at a cost of limiting audibility and possibly decreasing the benefits provided by a directional microphone.5 Furthermore, there is the potential degradation in sound quality from the interaction between the direct sounds and the amplified sounds. Logically, it will be beneficial to know the precise vent diameter so one may minimize occlusion while preserving intelligibility and sound quality. A simple approach is to select a vent diameter that is large enough to minimize as much occlusion as possible but not so large that the required gain in the high frequencies is compromised.
If one assumes that the average OE is 20 dB and that each 1 mm increase in vent diameter decreases the OE by about 4 dB, one would require a vent diameter of 5 mm to totally eliminate all occlusion effect. This is a very large vent and may not be feasible in most cases. On the other hand, that vent size may not be necessary if the hearing aid wearer can be taught to accept some degree of physical occlusion through counseling.6
Considering all the issues at hand, if the primary purpose is to optimize own-voice quality, with speech intelligibility being a close secondary objective, we would recommend:
• An open fitting for someone with a mild hearing loss and for someone with essentially normal hearing (less than 20 dB HL) at 500 Hz.
• Individuals with >20-30 dB HL at 500 Hz would require a vent diameter that is at least 3 mm wide.
• As the degree of hearing loss increases, the diameter of the needed vent decreases. In general, every 10 dB increase in hearing loss at 500 Hz would require a 0.5 mm decrease in vent diameter.
This recommendation assumes the average vent length (around second bend) and that active feedback cancellation is available on the hearing aid (decrease the vent diameter by 1 mm when active feedback cancellation is not available).

|
References
1. Kuk F, Keenan D, Peeters H. Ampclusion 103: Managing high frequency hearing loss. The Hearing Review. 2005;12(4):36-42.
2. Dillon H. Hearing aid earmolds, earshells and coupling systems. Hearing Aids. New York: Thieme Medical Publishers/Boomerang Press; 2001:117-157.
3. Mackersie C, Boothroyd A, Minniear D. Evaluation of the Computer-assisted Speech Perception Assessment Test (CASPA). J Am Acad Audiol. 2001;12(8):390-396.
4. Kuk F, Keenan D, Lau C. Vent configurations on subjective and objective occlusion effect. J Am Acad Audiol. 2005;16(9):747-762.
5. Kuk F, Keenan D, Sonne M, Ludvigsen C. Efficacy of an open fitting hearing aid. The Hearing Review. 2005;12(2):26-32.
6. Kuk F, Ludvigsen C. Ampclusion 102: A 5-step approach to remediation. The Hearing Review. 2002;9(9):34-43.
Correspondence can be addressed to HR or Francis Kuk, Widex Office of Research in Clinical Amplification, 2300 Cabot Dr, Ste 415, Lisle, IL 60532; email: [email protected].



