Research | September 2016 Hearing Review
Opening the door wider for the brain to receive the auditory signals it needs
Wireless connectivity in hearing aids is a powerful tool that offers significant potential communication improvement for hearing aid users. Such improvement can only be achieved when the end user is skilled in the use of wireless technology, and the hearing care professional has opened the doorway to the brain to the greatest extent possible. This is achieved through real-ear verified hearing aid programming, sufficient hearing aid use instruction, and description of the benefits and limitations of hearing aids and wireless technology.
Hearing aids, properly fit by hearing care professionals, must provide as much information to the brain as possible for every patient with hearing loss. In this context, a hearing loss might be considered a narrowing of the door to the brain. It then behooves the clinician to seek means by which this door can be opened to the greatest extent possible.
It is the thesis of this paper that wireless connectivity in hearing aids provides a major “door opener” for the person with hearing loss. As it relates to hearing aids, wireless connectivity refers to streaming acoustic signals from external microphones, telephones, sound systems, and media devices without the use of hard-wired cables.
The literature describing use of wireless connectivity in hearing aids usually follows three major areas of discussion:
1) Studies delineating the problems associated with the communication experiences of hearing aid users;
2) Studies showing that wireless connectivity in hearing aids addresses many of the problems that result in hearing aid user dissatisfaction, and
3) Studies on communication limitations not amenable to solutions by use of wireless connectivity in hearing aids.
The evidence that supports these three areas is as follows:
1) Problems Associated with the Communication Experiences of Hearing Aid Users
MarkeTrak IX shows that only 48% of 765 hearing aid owners in 2015 reported that hearing aids routinely improve their quality of life.1 In 2012, Kochkin2 noted that survey respondents reported hearing aids reduced their communication difficulty on the telephone, in meetings, at church, and in other noisy places by approximately 50%.
These two surveys, which collectively include over 3,000 hearing aid users, show that satisfaction with hearing aid performance on the telephone, in church, in classrooms, in meetings, and in other noisy places is unacceptably low. Clearly there is need for technology that improves these performance estimates.?It is our contention this technology is wireless connectivity in hearing aids.
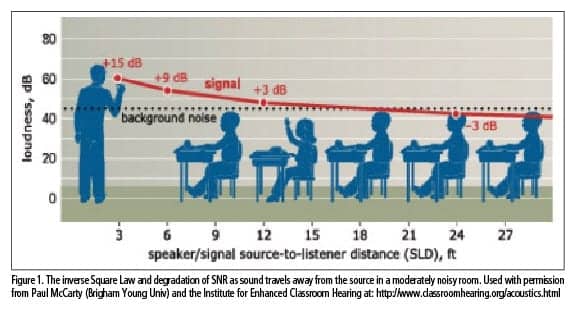
- Unfavorable signal-to-noise ratio,3-34
- Reverberation,3-7,9,14,21,22,30-46
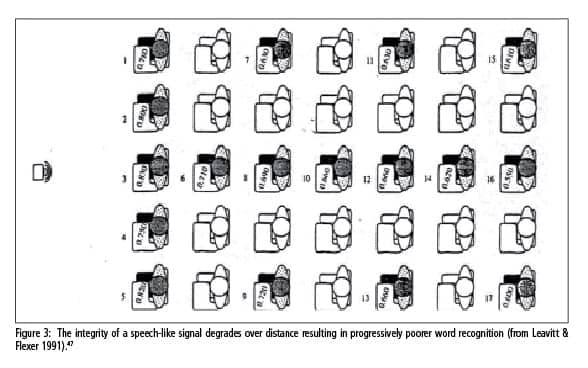
- Disproportionate degradation of high-frequency information,47 and
- Inverse Square Law effects.3,5,13,47,48
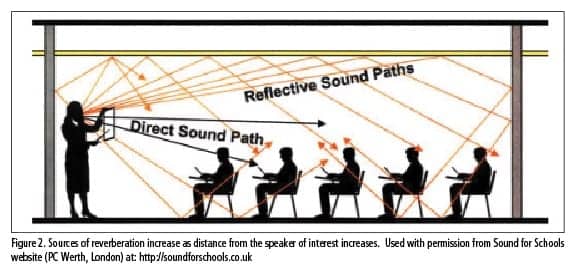
Figures 1-3 illustrate how these acoustic issues affect the speech understanding of a person with hearing loss in a classroom or meeting environment. These figures illustrate that sound pressure decreases markedly over distance, while background noise tends to be more constant.
2) Wireless Connectivity in Hearing Aids Addresses Many of the Problems Associated with Hearing Aid User Dissatisfaction
Benefits of a remote microphone. Wireless connectivity in hearing aids mitigates many of these aforementioned communication issues by use of a remote microphone. When a remote microphone is worn by the speaker, the background noise levels typically remain well below the signal of interest, the multiple sources of reverberation are reduced, the disproportionate dispersion of high-frequency energy is minimized, and the integrity of high-frequency speech sounds is maintained to a greater extent.49-59

The results show that an approximate gain of 20 dB was achieved at most frequencies when the remote microphone was placed 6 inches in front of the Axiom’s loudspeaker. Obviously, such increased gain creates a dramatically better SNR and an improved aided Speech Intelligibility Index (SII). Additionally, the effects of reverberation are minimized as the microphone is placed closer to the signal of interest where the effects of reverberation are less significant. Finally, the Inverse Square Law is largely overcome as is disproportionate degradation of high-frequency speech sounds traveling over distance.
As noted in the earlier analogy, the remote microphone “widens the doorway to the brain.”
Addressing telephone problems with wireless connectivity. As noted previously, satisfaction with telephone use is also relatively poor among hearing aid users. The reasons for this dissatisfaction stem from the difficulty associated with aligning the telephone earphone with the microphone of the hearing aid, from telecoil and phone compatibility issues, and from feedback concerns.
Numerous hearing aid manufacturers provide an intermediary device that receives a Bluetooth signal from an appropriately equipped telephone and transduces that signal into the hearing aid. It is of interest to assess how listeners with “golden ears” would rate these various telephone intermediary devices for sound quality, when the person with normal hearing listens from a landline phone to the intermediary device connected to a Bluetooth-enabled landline or cell phone.
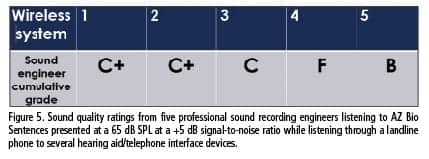
To test the sound quality of various manufacturers’ intermediary devices, 5 professional sound recording engineers were asked to give a letter grade to 5 different telephone interface devices while listening on a land-line phone in another room. These engineers were instructed not to judge the audio fidelity based on their studio monitors, but rather to base their ratings on the sound quality they typically receive from a landline telephone.
The speech signal was Az Bio Sentences presented at 65 dB SPL at a +5 dB SNR as measured at the microphone inlets of the telephone intermediary devices using an Extech 407780A sound-level meter. The sentences were produced by a Logitech loudspeaker placed at a 0° azimuth, with noise coming from 4 other Logitech speakers oriented at 70°, 140°, 210°, and 280° relative to the primary loudspeaker.
It is also of interest to measure speech recognition for the hearing aid user when using these various telephone intermediary devices. To this end, the fourth author (Carrie Rector) used 5 different telephone interface devices while listening to AZ Bio sentences. The test sentences came from a landline phone placed in another room. The Az Bio Sentences were presented at a 65 dB SPL at a +5 dB SNR as measured at the mouthpiece of the landline telephone. The Logitech speakers were placed at the same 0°, 70°, 140°, 210°, and 280° azimuths. She wore each of the applicable intermediary devices corresponding to the manufacturers’ hearing aids, and the aids were programmed to an NAL NL-2 target for 55, 65 and 70 dB SPL outputs based on her hearing loss.

As Figure 6 demonstrates, these manufacturers’ wireless interface devices do not provide equal speech recognition on the telephone for this listener. Consistent with these findings, the fourth author noted that she could not comprehend the sentences without guessing, except when wearing the hearing aid/telephone interface devices denoted as Systems 3 and 5 in Figure 6.
Of particular note in Figures 5 and 6 are the favorable sound quality ratings and word recognition scores obtained with System 5. This device transmits directly from an iPhone to the hearing aid with no intermediary device. It is suspected that the improvement in sound quality scores from the sound engineers with this device may be due to having one less data compression system—namely the intermediary device. Specifically, when an intermediary device is inserted between a Bluetooth-enabled phone and a hearing aid, the speech signal is compressed twice. First, the signal is compressed by the intermediary device, and then the transmission from the intermediary device to the Bluetooth enabled phone compresses the signal a second time.
These results also support the recent call for the establishment of sound quality and fidelity standards in wireless streaming hearing devices.60
3) Communication Limitations Not Amenable to Solutions via Wireless Connectivity in Hearing Aids
Wireless connectivity in hearing aids is not a panacea for all communication problems experienced by people using hearing aids. It is important for the hearing care professional to remember that, while wireless technology may dramatically improve communication in a variety of listening situations, there are numerous factors that may decrease the benefit of any wireless interface device.
For example, hearing aids that are under-fit can dramatically compromise word recognition, even when an external microphone is being used. Leavitt and Flexer61 showed that premium-level hearing aids cannot overcome communication problems in noise when these aids are under-fit relative to a well-established target. This problem of hearing aid under-fitting is compounded as the original default program of the hearing aid is typically the program used for wireless transmission. As such, it is possible that, even with the aforementioned advantages potentially provided by a remote microphone or a telephone interface device, insufficient gain provided in the default program will likely compromise the hearing aid user’s speech recognition.
In addition, patients with unrealistic hearing aid expectations, phonemic regression, central auditory processing problems, Auditory Neuropathy Spectrum Disorder, hearing aid use problems, hearing aid feedback issues, and/or cognitive problems may experience communication problems even when appropriate hearing aid targets have been achieved and wireless technology is working optimally.
While many of the aforementioned factors compromising hearing aid/wireless device benefit are outside the hearing care professional’s control, we can assure that appropriate amplification has been achieved through real-ear measures. Further, we can ascertain that wireless technology is not only functioning properly, but the hearing aid user is skilled in the manipulation of such technology.
Our ongoing goal must be to provide as much auditory information as possible to the brain of the person with hearing loss, in all listening environments. Achieving this goal requires a real-ear verified hearing aid output, a high fidelity wireless connection, and the skilled use of hearing aids and wireless technology by the end user.
As Cox, Johnson, and Xu62 noted, audiologists should focus on patient-centered training and appropriate individualized hearing aid programming. It is folly to assume that simply choosing hearing aids based on premium features and wireless connectivity will optimize speech intelligibility outcomes for our patients.
In short, wireless connectivity in hearing aids is a powerful tool that offers significant communication improvement for hearing aid users. Such improvement can only be achieved when the end user is skilled in the use of wireless technology and the hearing care professional has opened the doorway to the brain to the greatest extent possible. This is achieved through real-ear verified hearing aid programming, sufficient hearing aid use instruction, and description of the benefits and limitations of hearing aids and wireless technology.
References
-
Abrams HB, Kihm J. 2015; An Introduction to MarkeTrak IX: A new baseline for the hearing aid market. Hearing Review;22(6):16.
-
Kochkin S. 2012; MarkeTrak VIII: The key influencing factors in hearing aid purchase intent. Hearing Review. 19(3):12-25.
-
Finitzo-Heiber T, & Tillman TW. 1978; Room acoustics effects on monosyllabic word discrimination ability for normal and hearing-impaired children. J Speech Lang Hear Res. 21(3): 440–458.
-
Harris RW, Reitz ML. 1985; Effects of room reverberation and noise on speech discrimination by the elderly. Audiol. 24(5): 319-24.
-
Bradley JS. 1986; Speech intelligibility studies in classrooms. J Acoust Soc Am. 80(3): 846–854.
-
Irwin RJ, McAuley SF. 1987; Relationships among temporal acuity, hearing loss, and the perception of speech distorted by noise and reverberation. J Acoust Soc Am. 82(5): 1557-65.
-
Yacullo WS, Hawkins DB. 1987; Speech recognition in noise and reverberation by school-age children. Audiol. 26(4): 235–246.
-
Cox RM, Gilmore C. 1990;?Development of the Profile of Hearing Aid Performance (PHAP). J Speech Hear Res. 33(2):343–57.
-
Harris RW, Swenson DW. 1990; Effects of reverberation and noise on speech recognition by adults with various amounts of sensorineural hearing impairment. Audiol. 29(6): 314-21.
-
Helfer KS, Wilber LA. 1990; Hearing loss, aging, and speech perception in reverberation and noise. J Speech Hear Dis. 33(1): 149-55.
-
Helfer KS, Huntley RA. 1991; Aging and consonant errors in reverberation and noise. J Acoust Soc Am. 90(4pt1): 1786-96.
-
Blake P, Busby S. 1994; Noise levels in New Zealand junior classrooms: Their impact on hearing and teaching. New Zea Med J. 107(985): 357–358.
-
Crandell CC, Smaldino JJ. 1994; An update of classroom acoustics for children with hearing impairment. Volta Rev. 96(5): 291–306.
-
Helfer KS. 1994; Binaural cues and consonant perception in reverberation and noise. J Speech Hear Res. 37(2): 429-38.
-
Moore BCJ. 1995; Perceptual Consequences of Cochlear Damage. New York: Oxford University Press.
-
Moore BCJ. 2001; Identifying dead regions in the cochlea: diagnosis, perceptual consequences, and implications for the fitting of hearing aids. Trends Amplif. 24(2): 133-42.
-
Gatehouse S. 1999; Glasgow hearing aid benefit profile: derivation and validation of a client-centered outcome measure for hearing aid services. J Am Acad Audiol. 10(2): 80–103.
-
MacKenzie DJ, Airey S. 1999; Classroom Acoustics (Summary Report). Edinburgh, Scotland: Heriot-Watt University, Department of Building Engineering and Surveying.
-
Haines MM, Stansfeld SA, Job RF, Berglund B, Head J. 2001; Chronic aircraft noise exposure, stress responses, mental health and cognitive performance in school children. Psych Med. 31(2): 265-77.
-
Lukas JS. 2001; Noise, classroom behavior and third and sixth grade reading achievement.17th ICA Proceedings, Rome, 5, 144-145.
-
Picard M, Bradley JS. 2001; Revisiting speech interference in classrooms. Audiol. 40(5): 221-44.
-
Knecht HA, Nelson PB, Whitelaw GM, Feth LL. 2002; Background noise levels and reverberation times in unoccupied classrooms: Predictions and measurements. Am J Audiol. 11(2): 65-71.
-
Skarlatos D, Manatakis M. 2003; Effects of classroom noise on students and teachers in Greece. Percept Motor Skills. 96(2): 539-44.
-
Mackersie CL, Crocker TL, Davis RA. Limiting high-frequency hearing aid gain in listeners with and without suspected cochlear dead regions. J Am Acad Audiol. 2004;15:498–507.
-
Preminger JE, Carpenter R, Ziegler CH. A clinical perspective on cochlear dead regions: intelligibility of speech and subjective hearing aid benefit. J Am Acad Audiol. 2005;16:600–613. quiz 631-602.
-
Larsen JB, Blair JC. The effect of classroom amplification on the signal-to-noise ratio in classrooms while class is in session. Lang Speech Hear Serv Sch. 2008 Oct;39(4):451-60.
-
Shield BM, Dockrell JE. 2008; The effects of environmental and classroom noise on the academic attainments of primary school children. J Acoust Soc Am. 123(1): 133–144.
-
Bernstein JGW, Grant KW. 2009; Auditory and auditory-visual intelligibility of speech in fluctuating maskers for normal-hearing and hearing-impaired listeners. J Acoust Soc Am. 125(5):3358–72.
-
Walden TC, Walden BE, Summers V, Grant KW. 2009; A naturalistic approach to assessing hearing aid candidacy and motivating hearing aid use. J Am Acad Audiol. 20(10):607–20.
-
Yang W, Bradley JS. 2009; Effects of room acoustics on the intelligibility of speech in classrooms for young children. J Acoust Soc Am. 125(2): 922–933.
-
Neuman AC, Wróblewski M, Hajicek J, Rubinstein A. 2010; Combined effects of noise and reverberation on speech recognition performance of normal-hearing children and adults. Ear & Hear. 31(3):336-44.
-
Neuman AC, Wróblewski M, Hajicek J, Rubinstein A. 2012; Measuring speech recognition in children with cochlear implants in a virtual classroom. J Speech Lang Hear Res. 55(2): 532-40.
-
Gifford RH, Dorman MF, Skarzynski H, Lorens A, Polak M, Driscoll CL, Buchman CA. 2013; Cochlear implantation with hearing preservation yields significant benefit for speech recognition in complex listening environments. Ear & Hear. 34(4): 413–25.
-
Mason M, Kokkinakis K. 2014; Perception of consonants in reverberation and noise by adults fitted with bimodal devices. J Speech Lang Hear Res. 57(4): 1512-20.
-
Duquesnoy AJ, Plomp R. 1980; Effect of reverberation and noise on the intelligibility of sentences in cases of presbyacusis. J Acoust Soc Am. 68(2):537-44.
-
Neuman AC, Hochberg I. 1983; Children’s perception of speech in reverberation. J Acoust Soc Am. 73(6): 2145-9.
-
Náb?lek AK. 1988; Identification of vowels in quiet, noise, and reverberation: Relationships with age and hearing loss. J Acoust Soc Am. 84(2): 476-84.
-
Humes LE, Christopherson L. 1991; Speech identification difficulties of hearing-impaired elderly persons: The contributions of auditory processing deficits. J Speech Hear Res. 34(3): 686-93.
-
Gordon-Salant S, Fitzgibbons PJ. 1993; Temporal factors and speech recognition performance in young and elderly listeners. J Speech Hear Res. 36(6): 1276-85.
-
Gordon-Salant S, Fitzgibbons PJ. 1995; Comparing recognition of distorted speech using an equivalent signal-to-noise ratio index. J Speech Hear Res. 38(3): 706-13.
-
Halling DC, Humes LE. 2000; Factors affecting the recognition of reverberant speech by elderly listeners. J Speech Lang Hear Res. 43(2): 414-31.
-
Hedrick MS, Younger MS. 2007; Perceptual weighting of stop consonant cues by normal and impaired listeners in reverberation versus noise. J Speech Lang Hear Res. 50(2): 254-69.
-
Marrone N, Mason CR, Kidd G Jr. 2008; The effects of hearing loss and age on the benefit of spatial separation between multiple talkers in reverberant rooms. J Acoust Soc Am. 124(5): 3064-75.
-
Wróblewski M, Lewis DE, Valente DL, Stelmachowicz PG. 2012; Effects of reverberation on speech recognition in stationary and modulated noise by school-aged children and young adults. Ear & Hear. 33(6): 731–744.
-
Spitzer JB, Sandridge SA, Newman CW, Sydlowski S, Ghent RM Jr. 2015; A speech perception test in simulated reverberation conditions. Am J Audiol. 24(2):169-77.
-
Iglehart F. 2016; Speech Perception in Classroom Acoustics by Children With Cochlear Implants and With Typical Hearing. Am J Audiol. [Advance online publication], 1-10. Doi: 10.1044/2016_AJA-15-0064.
-
Leavitt R, Flexer C. 1991; Speech degradation as measured by the Rapid Speech Transmission Index (RASTI). Ear & Hear. 12(2): 115-8.
-
Rosenberg GG, Blake-Rahter P, Heavner J, Allen L, Redmond BM, Phillips J, Stigers K. 1999; Improving Classroom acoustics (ICA): A three-year FM sound field classroom amplification study. J Ed Audiol. 68(3): 283-93.
-
Hawkins DB. 1984; Comparisons of speech recognition in noise by mildly-to-moderately hearing-impaired children using hearing aids and FM systems. J Speech Hear Dis. 49(4): 409-418.
-
Boothroyd A, Iglehart F. 1998; Experiments with classroom FM amplification. Ear & Hear. 19(3): 202-217.
-
Pittman AL, Lewis DE, Hoover BM, Stelmachowicz PG. 1999; Recognition performance for four combinations of FM system and hearing aid microphone signals in adverse listening conditions. Ear & Hear. 20(4), 279.
-
Anderson KL, Goldstein H. 2004; Speech perception benefits of FM and infrared devices to children with hearing aids in a typical classroom. Lang Speech Hear Serv School. 35(2):169-84.
-
Schafer EC, Thibodeau LM. 2006; Speech recognition in noise in children with cochlear implants while listening in bilateral, bimodal, and FM-system arrangements. Am J Audiol. 15(2):114-26.
-
Chisolm,TH, Noe CM, McArdle R, Abrams H. 2007; Evidence for the use of hearing assistive technology by adults: The role of the FM system. Trends in Amp. 11(2):73-89.
-
Johnston KN, John AB, Kreisman NV, Hall JW, Crandell CC. 2009; Multiple benefits of personal FM system use by children with auditory processing disorder (APD). Int J Audiol. 48(6):371-83.
-
Purdy SC, Smart JL, Baily M, Sharma M. 2009; Do children with reading delay benefit from the use of personal FM systems in the classroom? Int J Audiol. 48(12):843-52.
-
Schafer EC, Wolfe J, Lawless T, Stout B. 2009; Effects of FM-receiver gain on speech-recognition performance of adults with cochlear implants. Int J Audiol. 48(4):196-203.
-
Hornich Zecker 2012
-
Thibodeau L. 2014; Comparison of speech recognition with adaptive digital and FM remote microphone hearing assistance technology by listeners who use hearing aids. Am J Audiol. 23(2): 201-210.
-
Ramsgaard J. Sound quality in hearing aid wireless streaming technologies. Hearing Review. 2016;23(8):24. Available at: https://hearingreview.com/2016/07/sound-quality-hearing-aid-wireless-streaming-technologies
-
Leavitt R, Flexer C. The importance of audibility in successful amplification of hearing loss. Hearing Review. 2012;19(12):20-23. Available at: https://hearingreview.com/2012/12/the-importance-of-audibility-in-successful-amplification-of-hearing-loss
-
Cox RM, Johnson JA, Xu. Impact of advanced hearing aid technology on speech understanding for older listeners with mild to moderate, adult-onset, sensorineural hearing loss. Gerontol. 2014;60(6):557-68.

Correspondence can be addressed to HR or Dr Leavitt at: [email protected].
Original citation for this article: Leavitt RJ, Flexer C, Clark N, Rector C. Unraveling the Mysteries of Wireless Connectivity in Hearing Aids. Hearing Review. 2016;23(9):14.?


Kudos to the authors for writing this article about the elephant in the room: that hearing aids are not very effective in situations where distance, reverberation and background noise are involved and that clients need to be educated on hearing aid microphone limitations and work arounds. The hearing aid is unique in the sense that it can receive acoustic signals– via the on board microphone, Bluetooth signals–when paired to a smart phone, TV or mini-mic transmitter AND magnetic signals when the telecoil is activated in a venue equipped with a telecoil [loop system].
This paper describes how moving a mini-mic from the ear of the listener to within inches of a real-ear equipment speaker, the signal-to-noise is dramatically improved. This is EXACTLY what happens in a hearing loop and I believe this article makes the PERFECT segue into the need for educating clients about telecoils and hearing loops. Hearing loops seamlessly provide direct hearing aid compatible assistive listening that greatly improve the users’ experience with their hearing devices.
Hearing Loops are amazingly beneficial to consumers. This was demonstrated in a recent survey http://www.hearingreview.com/2014/09/consumer-perceptions-impact-inductively-looped-venues-utility-hearing-devices/ where 866 people were asked to rate the performance of their hearing aids or cochlear implants using a 10-point scale. The average response was 4.9 in a non-looped setting and 8.7 in a looped environment. A second survey (unpublished data) polled listening effort on a 10-point scale (where 10 equaled “extreme effort” and 1 meant “no effort at all”) among some 300 users of a hearing loop at the annual Convention of Hearing Loss Association of America banquet, an event attended by over 630 people. Out of the loop the average listening effort was judged to be 6.9 and improved to 1.9 in the looped condition.
Good thing that the grassroots movement to make public facilities directly hearing aid compatible with telecoils through the use of hearing loops is growing by leaps and bounds. For more information on how to get your community in the loop visit http://www.loopwisconsin.com. To find looped places to send your clients to go and try, download the LoopFinder or LoopMyPhone apps available for free in the app store or visit http://www.aldlocator.com.