
Tech Topic | January 2022 Hearing Review
By David Crowhen, MAud
Step-by-step instructions for verifying CROS and BiCROS fittings using real-ear probe microphone verification (both REIG and SpeechMap methods).
Most clients of hearing care professionals (HCPs) present with bilateral, aidable hearing loss. However, some people have hearing loss in only one ear. Known as unilateral hearing loss (UHL), this can be defined as any degree of permanent hearing loss in one ear (PTA at 0.5, 1, 2 kHz > 15 dB) with normal hearing in the opposite ear.1
The incidence of UHL varies in the literature (possibly due to definition), with reports of 1 in 1,000 newborns identified with UHL at birth,2 3 in 100 children developing UHL by school age,3 and around 27 per 100,000 in adulthood.4 People with UHL may experience challenges communicating in noise, at a distance/for soft speakers, and when localizing sounds.5 And for children, these challenges can also impact on speech and language development6 and even performance at school.7 Along with UHL, where the affected ear is unaidable, some people may also develop hearing loss in the other ear, and this group will also be considered in this paper.
Advances in technology mean we now have more management options for UHL than ever before, and the optimal approach is dependent upon a number of factors relating to the hearing status in both ears and the client’s needs (Table 1). A discussion of all the possible approaches outlined in Table 1 is beyond the scope of this article which instead will focus on the options highlighted in green.
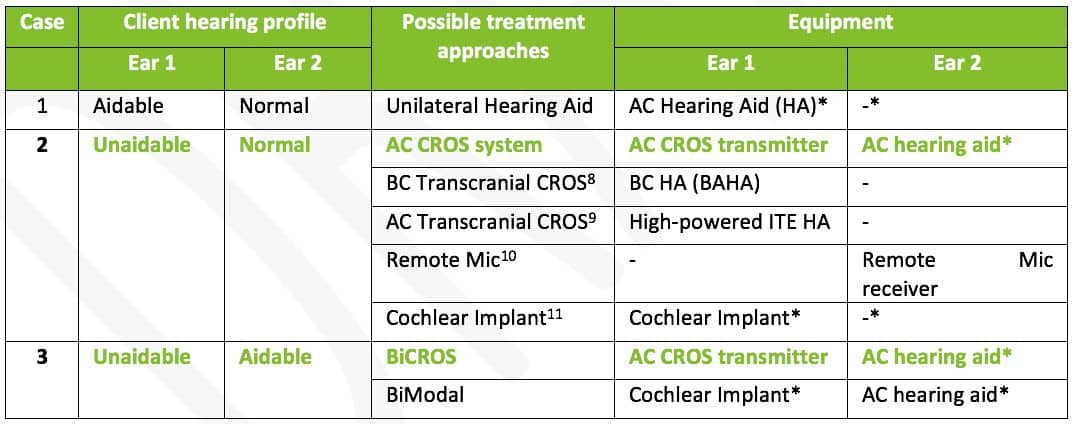
Table 1. Summary of the main treatment approaches for UHL as a function of different hearing profiles. Abbreviations: AC-Air Conduction; BC-Bone Conduction; HA-Hearing aid; CROS-Contralateral Routing of the Signal; BiCROS-Bilateral contralateral routing of the signal; BAHA-Bone- anchored hearing aid; ITE-In the ear. Systems with an asterisk (*) may also benefit from a remote mic system in this ear as well.
Unaidable hearing in one ear with normal hearing in the other ear. A common approach for managing clients with unaidable hearing in one ear and normal hearing in the other is to fit them with a Contralateral Routing of Signals, or CROS, system.12 In a CROS fitting, a device is worn behind both ears, and the signal is wirelessly transmitted from the unaidable ear and presented to the normal ear. Because the hearing in the better ear is normal, little or no amplification is provided to the crossed signal as the concept is simply to overcome the head-shadow effect.13
Unaidable hearing in one ear, aidable hearing loss in the other ear . For patients with UHL who also have a hearing loss in their better-hearing ear, a Bilateral Contralateral Routing of Signals, or Bi-CROS solution is more suitable.5 In a Bi-CROS system, again, a device is worn behind both ears, and the signal from the unaidable ear is wirelessly transmitted to the better ear. However, because there is a hearing loss in the better ear, this signal is amplified according to the gain requirement for hearing loss in this ear. Concurrently, information picked up from the microphone on the better-hearing side is similarly amplified. So, in a BiCROS system, both the head-shadow effect and reduced hearing sensitivity on the better-hearing side are ameliorated.
The Role of Probe-Mic Measures in Verifying CROS/Bi-CROS Fittings
While the benefits of binaural amplification for clients with aidable hearing loss in both ears are often immediately evident, they may initially be more subtle for those with unusable UHL and normal/near normal hearing in the other ear.Indeed, Mueller and Hawkins14 reported that these patients sometimes find it challenging to reliably report whether their CROS system/transmitter is operational. Thus, probe microphone measures present an ideal, objective way for verifying that a CROS/Bi-CROS system is functioning well and overcoming the head-shadow effect.15 Further support for utilizing probe-mic measures when fitting hearing aids comes from MarkeTrak findings, showing those patients receiving best-practice fittings experience greater reduction in hearing handicap compared to those who don’t,16 and that patients who received both verification and validation measures required on average 1.2 less visits compared to those who did not.17
Accordingly, this paper aims to provide an easy, step-by-step guide for performing probe-microphone measures to verify CROS/BiCROS fittings in a practice. This guide is based on the outline provided by Pumford15 and assumes the real-ear measurement (REM) machine has the ability to switch reference microphones across ears while measuring output in the better ear. This ensures accurate stimulus calibration at all steps of the procedure.
CROS Fittings
To illustrate the method for verifying CROS fittings using probe-microphone measures, consider this case of a male who, at age 16, had a sudden profound sensorineural hearing loss and commensurately poor speech discrimination in the right ear, with normal hearing in the left ear (Figure 1).

Figure 1. Pure-tone audiogram showing profound hearing loss on the right ear and normal hearing on the left.
He persevered with this UHL during his final years in secondary/high school, but since starting university has found it very difficult to hear fellow students on his right side during lectures/tutorials. He also drives an Uber part time and has difficulty hearing passengers in the front seat (right-hand driving lane). His clinician decided to fit him with an Audéo P90-R and open fitting on the left ear, and a CROS P-R transmitter on the right.
Summarized in Figure 2, are the steps used to set up and verify the fitting using both the real-ear insertion gain (REIG, left screenshots) and SpeechMap methods (right screenshots).
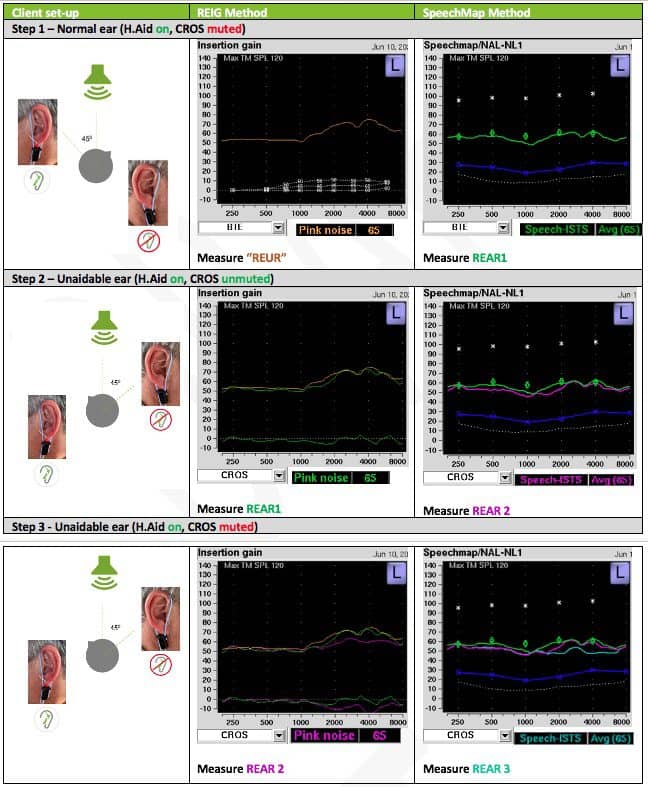
Figure 2. Steps for verifying a CROS fitting using the REIG method. REUR=Real-ear unaided response; REAR1=Real-ear aided response #1; REAR2= Real-ear aided response #2, etc. *An angle of between 45° and up to 90° can be used, as shown in the left side of each panel.
Step 1: Place the REM reference microphones on both ears; however, only insert a probe mic into the better-hearing ear (this is the only ear we will be measuring hearing aid output from). Select <BTE> in the REM system instrument menu. Note there is no need to enter pure-tone thresholds into the REM system, as we are not trying to match hearing instrument gain/output to prescription targets as the hearing sensitivity is normal.
Place the Audéo P-R and CROS P-R on the normal and unaidable ear, respectively, and connect to Phonak Target. Activate the hearing aid but leave the CROS muted (do not select the Verification mode in Phonak target, as this will disable communication between the CROS and hearing aid). Orient the better-hearing ear to at least a 45° (and no greater than 90°) angle facing the REM speaker (Figure 2, Step 1).
For the REIG method, record the real-ear unaided response (REUR) of the better-hearing ear at a stimulus level of 65 dB SPL, which should look typical given the coupling is open/non-occluding. (Note: Technically, this isn’t a REUR, as the device is in the ear; we are simply recording a REUR so, when the subsequent real-ear aided response (REAR) is recorded, the difference between the two results in the REIG curve, which ideally will be approximately 0 dB across the frequency range). For the SpeechMap method, record a REAR1 for a 65 dB SPL stimulus.
Step 2: Unmute the CROS P transmitter system, change the orientation of the client so their unaidable ear is now oriented to at least a 45° (and no greater than 90°) angle facing the REM speaker (Figure 2, Step 2). Importantly, change the instrument type in the REM system to <CROS>. This disables the reference microphone on the better-ear side and activates the reference microphone on the unaidable side. If this is not done, the REM system will, through concurrent equalization, increase the stimulus level to overcome the head attenuation of the stimulus arriving at the reference microphone on the good side, and your output on the CROS side will be artificially high.
Once changed to <CROS>, for the REIG method, run a REAR1 curve at the same stimulus level (65 dB SPL). The REUR and REAR1 curves should be similar, resulting in a REIG of ~0 dB across the frequency range. For the SpeechMap method, run a REAR2 at the same stimulus level (65 dB SPL), and this should be similar to REAR1. It’s important to note that it’s very rare to see a perfect match (0 dB REIG), but it should be reasonably close.
If the output when the stimulus presented to the CROS transmitter is substantially lower than REUR on the REIG method/REAR1 on the SpeechMap method, try increasing the gain at relevant frequencies and/or adjusting the CROS balance tool to try and match more closely (see Figure 3a-b, top and bottom).

Figure 3. For CROS fittings where the output from the CROS side is lower than the normal/near-normal side, try: A) Increasing the gain in relevant frequency regions, and/or B) Adjusting the CROS balance tool.
It’s important to note that it is the gain settings that dictate the absolute output level in the better ear, whereas the CROS balance adjusts the relative contribution of the CROS and hearing aid microphones to that output. In my experience, large adjustments should not be required. At this point, I also recommend a subjective check on loudness balance across ears using a soft high-frequency sound (eg, live-voiced /s/). The reason to use a soft, high-frequency stimulus is because the head-shadow effect predominantly affects frequencies above 1500 Hz,18 and we are only wanting to test the influence of the equipment here—and not confound our validation with low frequencies, which will bend around the head and sound louder in the better-hearing ear.
Step 3: Finally, for both methods, with the client still in the same position as in Step 2 (ie, unaidable ear facing towards the REM speaker), mute the CROS transmitter and capture another curve (for REIG method – REAR2, for SpeechMap method, REAR3 and still using <CROS> in the REM system). This results in a curve that should fall below the two other curves; the difference between this curve and the two previous curves reflects the head shadow effect (Figure 2, Step 3).
BiCROS Fittings
To illustrate the method for verifying BiCROS fittings, consider this case of a 52-year-old male who had longstanding mild-moderate hearing loss bilaterally which he tolerated. Unfortunately, he sustained a viral infection which led to a sudden decline in hearing on the right to profound loss levels (Figure 4), converting his previously annoying, but tolerable, hearing issues into a major burden for him and his family. Therefore, a BiCROS fitting was recommended using a Audéo P90-13 on the left ear with a vented dome and a CROS P-13 on the right.
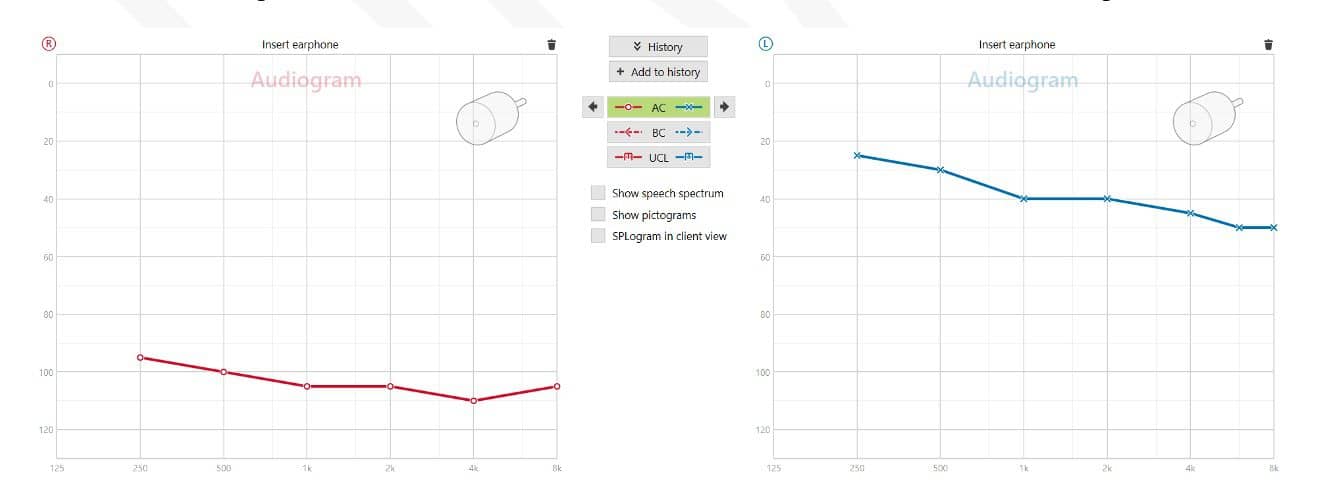
Figure 4. Pure-tone audiogram showing profound hearing loss on the right and mild-moderate sloping hearing on the left.
Step 1: For BiCROS fittings, the only difference compared to the above approach for verifying a CROS fitting is to first tune the hearing aid output according to the prescription targets and sound preference to ameliorate the hearing loss in the better-hearing ear. This is indicated in Figure 5, Step 1.
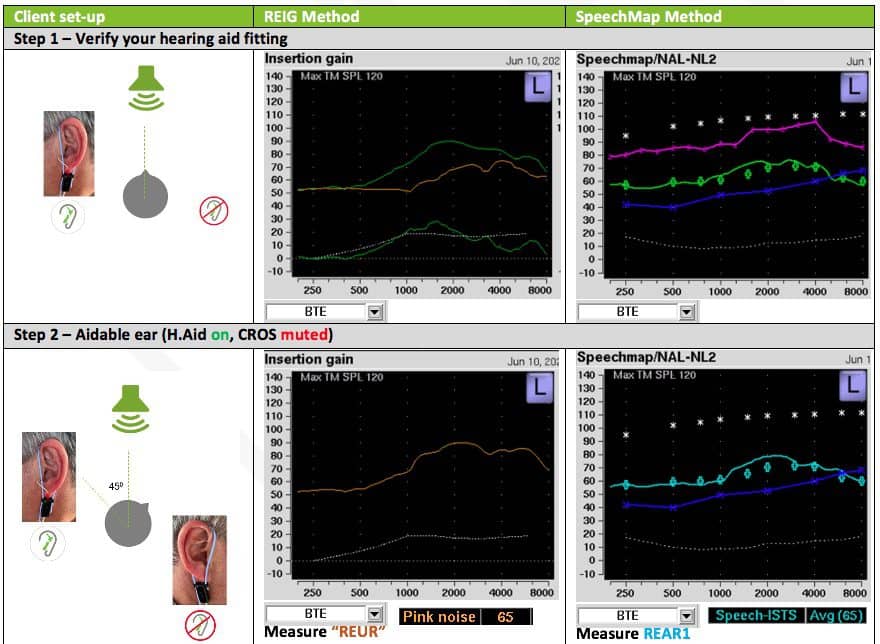
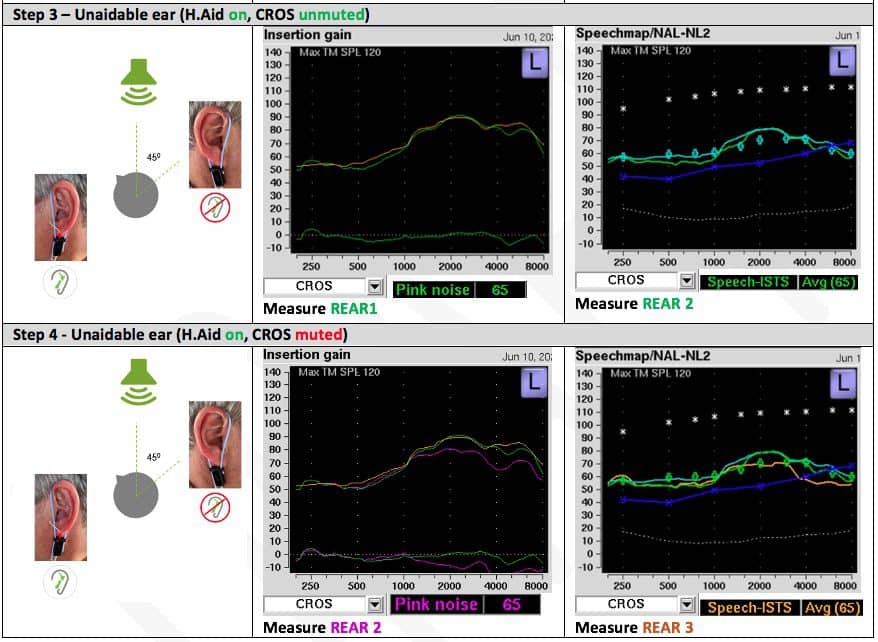
Figure 5. Steps for verifying a BiCROS P fitting using the REIG method. REUR=Real-ear unaided response, REAR1=Real-ear aided response #1, REAR2= Real-ear aided response #2, etc. *An angle of between 45° and up to 90° can be used.
Step 2: Following this, the procedure is identical to verifying the CROS system.
Steps 3-4: If, at Step 3, the output is lower when the stimulus is presented to the CROS transmitter (because we have already established suitable/preferred gain for ameliorating the hearing loss in Step 1), I would suggest only adjusting the CROS balance tool (see Figure 3b) to balance/match the curves. Similarly, I suggest cross-checking the objective probe-microphone measures by presenting a low-level high-frequency stimulus (eg, live voiced /s/) on both sides to determine subjective balance and, if necessary, adjust as already described.
Summary
Probe microphone measures provide an easy, objective, and reliable way to verify your CROS and Bi-CROS fittings. You can use either the REIG or SpeechMap method, depending on your preference and/or which one you are most familiar with.

CORRESPONDENCE to David Crowhen at: [email protected].
Citation for this article: Crowhen D. Optimizing CROS/BiCROS benefit using probe microphone verification and the Phonak CROS P. Hearing Review. 2022;29(1):22-25.
References
- Bagatto M, DesGeorges,J, King A, et al. Consensus practice parameter: Audiological assessment and management of unilateral hearing loss in children. Intl J Audiol. 2019; 58(12):805-815.
- Prieve B, Dalzell L, Berg A, et al. The New York State Universal Newborn Hearing Screening Demonstration Project: Outpatient outcome measures. Ear Hear. 2000;21(2):104–117.
- Bess, FH, Dodd-Murphy J, Parker RA. Children with minimal sensorineural hearing loss: Prevalence, educational performance, and functional status. Ear Hear. 1998;19(5):339-354.
- Alexander TH, Harris JP. Incidence of sudden sensorineural hearing loss. Otol Neurotol. 2013; 34(9):1586-1589.
- Dillon H. Hearing Aids. 2nd ed. Thieme;2012.
- Ead B, Hale S, DeAlwis D, Lieu JEC. Pilot study of cognition in children with unilateral hearing loss. Intl J Ped Otorhinolaryngol. 2013;77(11):1856-1860.
- Bess F,H Tharpe AM. Case history data on unilaterally hearing-impaired children. Ear Hear. 1986;7(1):14-19.
- Hol MKS, Kunst SJW, Snik AFM, Cremers CWRJ. Pilot study on the effectiveness of the conventional CROS, the transcranial CROS and the BAHA transcranial CROS in adults with unilateral inner ear deafness. Eur Arch Otorhinolaryngol. 2010; 267:889–896.
- Hayes DE, Chen JM. Bone-conduction amplification with completely-in-the-canal hearing aids. J Am Acad. Audiol. 1998;9(1):59-66.
- Kenworthy OT, Klee T, Tharpe AM. Speech recognition ability of children with unilateral sensorineural hearing loss as a function of amplification, speech stimuli and listening condition. Ear Hear. 1990;11(4):264-270.
- Sladen DP, Carlson ML, Dowling BP, et al. Early outcomes after cochlear implantation for adults and children with unilateral hearing loss. Laryngoscope. 2017;127(7):1683-1688.
- Harford E, Barry F. A rehabilitative approach to the problem of unilateral hearing impairment: The contralateral routing of signals (CROS). J Speech Hear Dis. 1965;30(2):121-138.
- Courtois G, et al. Hearing aid fitting in asymmetrical hearing loss. In: Jensen JH, ed. Hearing Aid Fitting: Theoretical and Practical Views Proceedings of the 13th Danavox Symposium Fjord.1988:243-256.
- Mueller HG, Hawkins DB. Assessment of fitting arrangements, special circuitry, and features. In: Mueller HG, Hawkins DB, Northern JL, eds. Probe Microphone Measurements: Hearing Aid Selection and Assessment. Singular;1992:201-225
- Pumford J. Benefits of probe-mic measures with CROS/Bi-CROS fittings. Hear Jour. 2005;58(10):34-40.
- Kochkin S. MarkeTrak VIII: Patients report improved quality of life with hearing aid usage. Hear Jour. 2011;64(6):25-32.
- Kochkin S. MarkeTrak VIII: Reducing patient visits through verification and validation. Hearing Review. 2011;18(6):10-12.
- Pickles JO. An Introduction to the Physiology of Hearing. 2nd ed. Emerald Group Publishing Ltd;1988.



