Tech Topic//Tinnitus | September 2015 Hearing Review
Previous studies have demonstrated the benefits of fractal tones and Widex Zen Therapy (WZT) when used in conjunction with amplification, but there have been no studies on the use of fractal tones alone (eg, without amplification) for tinnitus sufferers who do not require or wish to consider amplification. Results from this study strongly support the use of Zen alone, and of the integrated WZT approach in tinnitus patient management.
The effectiveness of amplification for hearing impaired tinnitus sufferers has been well documented.1-5 In fact, the 2014 AAO-HNS Clinical Practice Guidelines for Tinnitus6 “recommend a hearing aid evaluation for patients who have persistent, bothersome tinnitus associated with documented hearing loss.” In making its recommendation, the AAO-HNS development group reported that 17 of 18 reviewed trials showed benefit with hearing aid use, but it acknowledged (page S20) “the general low quality of evidence.”
Justifiable criticisms of many of these studies have been the lack of inclusion of a control group and the lack of long-term follow up.6 Moreover, despite the fact that the vast majority of tinnitus sufferers show some degree of auditory impairment, not all have sufficient hearing loss to warrant the purchase and use of hearing aids.
Therefore, several other “non-amplified” sound therapy options have been proposed. They include: narrow band noise (for masking purposes), broadband noise (for habituation), modulated noises, and/or filtered music. However, the effectiveness of steady state signals has been questioned,7 and a potential limitation of recorded music is the familiarity, which can produce active, rather than passive, listening.8 Moreover, repetitive music passages can potentially be retained in memory and either cause boredom, or unwanted memory repetitions, known as earworms.9
Thus, fractal tones have been employed as an alternative that achieves the benefits, but avoids the potential drawbacks of music. Fractals are tones with harmonic and semi-predictable relationships generated by a recursive process. The tones are pleasant, follow the “rules” governing relaxing music,10 but are not associated with tunes that the listener may hold in memory.
Multiple studies have demonstrated that the use of fractal tones combined with amplification can be effective in reducing tinnitus distress in tinnitus sufferers with a hearing loss. For example, a survey of patients who had been fitted with hearing aids containing fractal tones indicated that 69% had reductions in their Tinnitus Reaction Questionnaire (TRQ) scores of greater than 20 points.11 Changes in the Tinnitus Handicap Inventory (THI) and TRQ over a 6-month period following the fitting of hearing aids with fractal tones for subjects who had undergone previous tinnitus treatments with no success, found 36% of subjects showed THI improvements in excess of 20 points and 29% showed a 40% or greater improvement in the TRQ.12 Another investigation reported on 48 subjects receiving similar treatment with an average improvement in TRQ scores of approximately 60%.13
The previous studies demonstrated the benefits of the fractal tones when they were used in conjunction with amplification. There have been no studies on the use of fractal tones alone (eg, without amplification) for tinnitus sufferers who do not require or wish to consider amplification. Such studies are desirable because they would establish the effectiveness of fractal tones alone as an independent treatment option.
Most authors have suggested that sound stimulation (amplification and/or other sound stimuli) by itself is not adequate for patients who have significant negative reactions to the unwanted, auditory perception of tinnitus. Consequently, most tinnitus management approaches employ a substantial counseling component focused on demystifying the patient’s reaction to tinnitus or identifying maladaptive thoughts and behaviors and replacing them with alternative strategies. Cognitive behavioral therapy (CBT) is recommended in the 2014 AAO-HNS Guidelines for “patients with persistent, bothersome tinnitus.” In addition, given the well documented correlation between stress, insomnia, and tinnitus perception,14,15 the use of relaxation procedures and sleep management have been suggested.
An approach that integrates all of the above—instructional counseling, adjustment-based counseling (in the form of Cognitive-Behavioral Intervention), amplification (when appropriate), fractal tone stimulation (Zen) for stress reduction, and relaxation exercises (including sleep management)—was introduced and marketed as Widex Zen Therapy (WZT).16 WZT is an integrated program aimed at addressing the major contributors to tinnitus distress: auditory perception, heightened attention, and negative emotion. The different components of the WZT may be used in isolation or in combination, sequentially or simultaneously depending on the patient’s needs and progress.
Study Purpose
The objectives of this study were: 1) to determine if subjects with significant tinnitus whose hearing levels are either normal or mild enough that they do not perceive the need for amplification would benefit from a wearable device containing fractal tones and noise; 2) to compare progress in diminishing tinnitus distress with a control group receiving only instructional counseling; 3) to investigate whether additional components of an integrated approach to tinnitus management would be beneficial in serving this patient population, and 4) to determine the long-term effects 6 months after treatment ended.
Study Design
This investigation was performed at Widex in Lynge, Denmark with two groups of subjects. One was a treatment group using a behind-the-ear tinnitus device (Zen2Go) and WZT, and the other was a control group receiving only instructional (educational) tinnitus counseling. The treatment group’s intervention was divided into 2 phases. In Phase 1 (initial 2 months) the effects of sound stimulation with the fractal tones alone and instructional counseling were investigated. In Phase 2 (next 4 months) the effects of combining additional WZT components (amplification, cognitive behavioral intervention, relaxation, and sleep management)17 with sound stimulation were examined.
Subjects. Subjects were recruited via the Internet. Forty-one subjects enrolled initially. The first 19 subjects (mean age 51 years) were assigned to the treatment group. The next 22 subjects (mean age 50 years) seen at the clinic were assigned to the control group. All subjects met the inclusion requirements (medical clearance; clinically significant level of tinnitus-related disturbance; THI > 18); primary complaint of tinnitus with no acknowledgement of hearing loss that warranted the use of hearing aids; no cognitive deficits, and tinnitus duration of one year or more.
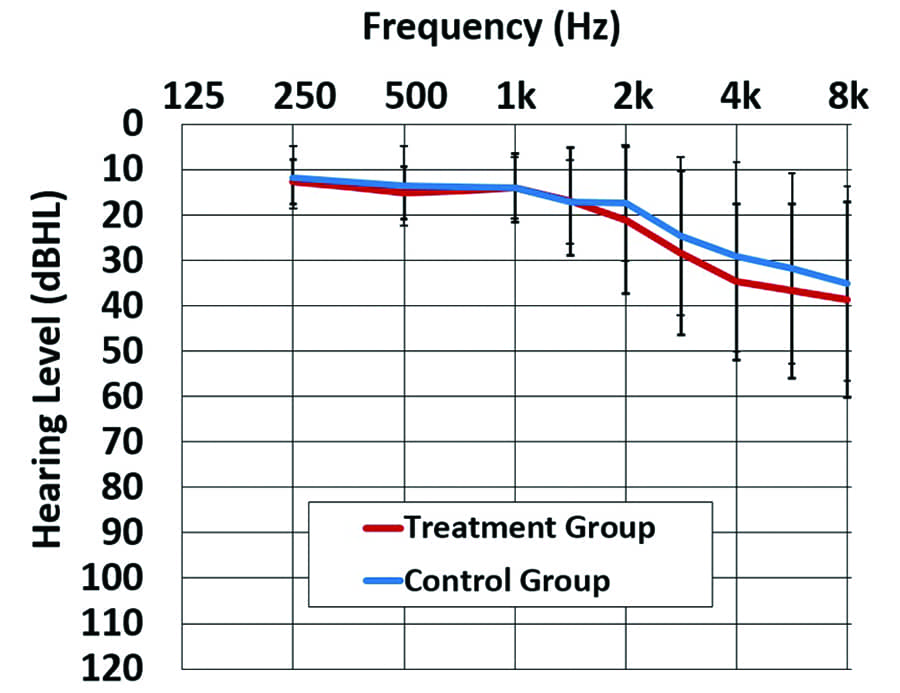
Figure 1. Mean thresholds and one standard deviation for the treatment group and the control group.
All subjects completed a comprehensive audiological and tinnitus evaluation. Most had normal hearing thresholds (25 dB HL or better) below 2 kHz. Some had slight hearing losses at high frequencies. None expressed the need or desire for amplification. Data collection was completed on 36 subjects. Three subjects in the treatment group and 2 subjects in the control group withdrew before the data completion. Figure 1 shows the mean hearing thresholds for both groups.
The treatment group had a mean THI score of 40, ranging from 22 to 92, while the control group’s mean THI score was 36, ranging from 18 to 78. The mean subjective estimate of loudness and pitch (based on a 10 point scale) for both groups were identical (loudness mean = 6, pitch mean = 8). Only 7 of the 36 final subjects indicated having received other tinnitus treatments previously. The nature of the tinnitus sounds varied, but hissing, whistling, and ringing were most often reported.
Study Device. The Widex Zen2Go device was used to provide the fractal tones used in sound stimulation. This is a miniature receiver-in-the-canal (RIC) style hearing aid that is specifically earmarked for tinnitus patients who do not consider the use of amplification necessary or beneficial. This includes tinnitus patients with normal hearing and those with a mild-to-moderate degree of hearing loss. Functionally, the Zen2Go device is identical to a Widex DREAM passion hearing aid, except that the default setting of the Zen2Go is just the Zen+ program with NO amplification. If it is later decided that the tinnitus patient may benefit from the use of amplification, this can be achieved by re-programming the device and activating the microphone switch. In the Zen+ program, subjects can cycle through three custom programs. In this study, program A included only the fractal tones. Program B included the fractal tones and filtered broadband noise, while program C included only the broadband noise option. Zen + aqua (program A) was recommended for quiet situations. Zen + noise (program B) or Zen noise alone (program C) were recommended during periods when clients experienced bothersome tinnitus.
Measurement Tools. The Tinnitus Functional Index (TFI)18 and THI19 were administered as the principal measurement tools in the study. Scores were collected at baseline, 2, 4, 6 (end of treatment) and 12 months (6 months following the end of treatment). The treatment group also completed measures at 1 month post-fitting.
Procedures. All subjects from both groups were given 90 minutes of detailed instructional counseling including epidemiology; reassurance that tinnitus is not life threatening; basic anatomy and physiology; relationship between auditory damage and tinnitus; relationship of tinnitus to emotional state (limbic system) and overall distress; feedback loop between negative reaction and increased tinnitus perception; description of why the perceptual characteristics of the tinnitus (eg, loudness) does not correlate directly with the magnitude of distress; explanation of the natural process of habituation, and barriers to that process.
The control group subjects were only required to attend the initial evaluation and instructional counseling session. They then completed (either in person or via mail) the follow-up outcome measures.
Subjects in the treatment group underwent one or two phases of treatment depending on their responsiveness to the Zen stimulus. Added sessions were provided when additional WZT components were included. In all, the treatment group attended at least 5 sessions: the fitting of Zen2go device(s), and follow up visits at 1, 2, 4 and 6 months.
Phase 1 (Sound stimulation with fractal tones). All subjects in the treatment group were fitted with the Zen2Go at the default settings. They were provided with the three Zen+ programs without amplification (even though some had measurable hearing loss in the high frequencies). Subjects were instructed to use Zen as much as needed and to not change the volume during the day.
Phase 2 (Sound stimulation and WZT). Eight of the total 16 subjects achieved criterion tinnitus reduction using fractal tones (Zen) alone at the end of Phase 1. Of these 8 subjects, 5 had normal hearing and 3 had a mild-to-moderate hearing loss. These 3 subjects were provided amplification despite reaching criterion tinnitus reduction. The remaining 8 subjects whose THI or TFI scores continued to exceed 18 at the 2nd follow up visit were provided with remaining components of the WZT protocol. Three of these 8 subjects had a mild-to-moderate hearing loss in the high frequencies. They were provided with amplification + cognitive behavioral intervention + relaxation exercises, in addition to Zen. The remaining 5 required Zen + cognitive behavioral intervention and relaxation only. Relaxation techniques included progressive muscle relaxation, deep breathing, and guided imagery. Subjects with sleep issues were provided strategies and used the Zen program at night (set to limited play time). One third of treatment subjects wore their devices to assist them in falling asleep.
Results
Tinnitus Distress Measures. There were positive correlations for both groups (p<0.001) between TFI and THI at all visits, strongly suggesting that both subjective scales were providing equivalent measures. Therefore, in the interest of brevity, only the TFI results are shown and discussed here.

Figure 2. Mean TFI scores at baseline, 2, 4, 6, and 12 months. Bars represent one standard deviation.
Figure 2 shows changes in the TFI scores. The mean TFI for the treatment group improved from a baseline score of 38, (range 18 to 70) to an end of treatment score of 17, (range 0 to 43). Thus, the mean improvement was 21 points. For the control group, the mean score changed from 45 (range 14 to 87) to 42 (range 12 to 80). Thus, the mean improvement for the control group was 3 points. Factorial repeated measures ANOVA revealed that visit was a significant factor (p<0.001) and the interaction between group and visit over time was also significant (p<0.001). A statistically significant difference between treatment and control groups was found (p<0.01).
Post-hoc analysis with Bonferroni adjustments for multiple comparisons using a paired-samples t-test also showed statistically significant changes at the 2, 4, and 6 month visits from baseline (p<0.001) in the treatment group. A clinical and statistical significant improvement of 21 points was found after only 2 months. Although TFI scores continued to improve between the 2, 4 and 6 month follow up visits in the treatment group, the difference was not statistically significant (p>0.05). No significant improvements occurred in the control group at any time (p>0.05). In addition, 75% of the treatment subjects had clinically significant changes in TFI scores (defined as more than 13 points in the treatment group versus only 15% in the control group.
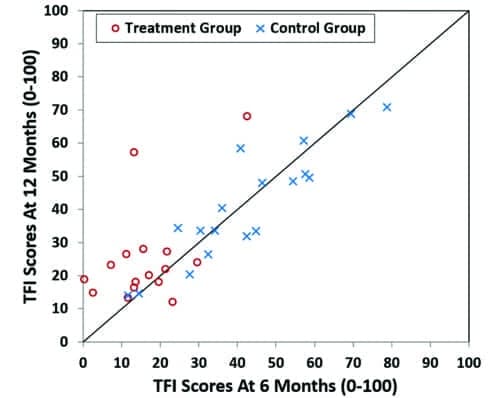
Figure 3. Individual TFI scores at 12 months (or 6 months post-treatment, vertical axis) versus TFI scores at end of treatment (or 6 months, horizontal axis) for the treatment and control groups.
Mean values for TFI increased slightly between the end of active treatment (6 months) and the follow up 6 months later. However, these changes were not statistically significant (p>0.05) and the differences between baseline measures and the 12 month data remain highly significant (p<0.001). Looking at individual data, it can be seen (Figure 3) that the majority of subjects maintained or improved their TFI scores during the 6 month period following treatment.
All WZT components versus sound therapy (Zen) + instructional counseling. One of the objectives of this study was to determine whether the additional components of an integrated approach to tinnitus management would be beneficial in serving this “normal hearing” tinnitus patient population. Recall that 8 subjects in the treatment group whose THI scores continued to be significant (exceeding 18) after the 1st phase of treatment (Zen only) were given additional WZT components (amplification, CBI and/or relaxation). Three of these 8 subjects were candidates for amplification. When the treatment group was subdivided into those receiving Zen + instructional counseling only versus subjects receiving the additional WZT components (amplification, Zen, CBI, relaxation exercises), both sub-groups demonstrated statistical and clinically significant improvement, though the differences between the two groups were not statistically significant (p>0.05).
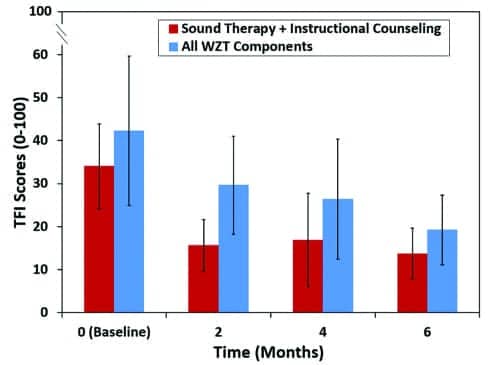
Figure 4. Mean TFI scores at baseline, 2, 4 and 6 months for the 2 treatment sub-groups. Bars represent one standard deviation. Significant improvements were seen in both groups (p<0.001).
It should be noted however, that, as expected, subjects in the sound therapy (Zen) + instructional counseling only sub-group presented lower initial baseline and subsequent TFI scores than the subjects who received additional WZT components (Figure 4). Furthermore, it is interesting to note that the most significant improvement occurred for the sound therapy (Zen) + instructional counseling group within the first 2 months, whereas the more distressed group receiving the additional WZT components showed a slower, but equally significant change throughout the first 6 months.
Discussion
This study was the first to investigate the efficacy of Zen (in the Zen2Go) and Widex Zen Therapy in reducing tinnitus distress for patients with normal (or perceived normal) hearing. In addition, it was the first to compare WZT effectiveness with a control group receiving instructional counseling only. The data revealed significant benefit within the first 2 months for the treatment group, with further (albeit not statistically significant) changes occurring through 6 months. The average reduction in TFI scores was 20 points (15.5 points after only 2 months). These differences were both statistically and clinically significant. No significant improvements were seen in the control group who received the same instructional counseling only. While other tinnitus treatments have reported similar magnitude of success,20, 21 the speed in which Zen2Go combined with WZT treatment achieved these changes is particularly impressive and critical, considering the importance of early success in maintaining motivation for tinnitus patients.

Robert W. Sweetow, PhD
Given that most tinnitus studies (including the previous published studies on WZT) have focused on hearing impaired subjects with tinnitus, it is of interest to compare the changes in tinnitus distress shown by the current “normal” hearing tinnitus subjects versus the hearing-impaired tinnitus subjects undergoing WZT in previous studies. In a 2014 study,22 the TFI improved by 28 points. In a 2015 study,23 the mean TFI improvement after 6 months of active treatment was 40 points. In the current study, the mean improvement in the same time frame was 22 points. It is possible that this difference in improvement is related to the starting baseline score. In the 2014 study,22 the TFI baseline was 53. In the 2015 study,23 the pre-treatment TFI score for the hearing-impaired tinnitus subjects was 60. In the current study, the “normal” hearing tinnitus subjects had a baseline TFI score of 38. In addition, it is possible that the larger magnitude of improvement in the 2014 study was related to the fact that all treatment subjects received amplification, whereas only 6 of the subjects in the current study received amplification.

Francis Kuk, PhD
It has been suggested that the favorable results obtained with sound therapy treatment may be mediated from the counseling and not necessarily from the acoustic stimulation itself.24 The data from this investigation suggest that instructional counseling alone is not sufficient; and instructional counseling plus the Zen stimuli alone was more effective in reducing tinnitus distress in sufferers with normal hearing. For sufferers who also have a concomitant hearing loss, the use of Zen plus amplification produced additional relief from tinnitus distress. The combination of the various components of the WZT integrated approach contributed to success with more distressed subjects.

Sueli Caporali, PhD
The longer-term benefit of tinnitus treatment was assessed 6 months after the end of active treatment. There was a slight increase in tinnitus distress scores in the treatment group, but they were not statistically significant. Analysis of the individual data showed that 3 of the 4 subjects whose tinnitus distress worsened did not use the tinnitus device after the end of treatment (6 months). Seven of the 8 subjects that continued using Zen2Go maintained the benefit obtained with the treatment after 12 months. This suggests that continued use of fractal tone/amplification sound therapy may be necessary to maintain the long-term benefit obtained with treatment for some patients.
Conclusions
Answers to each of the aforementioned objectives are summarized below:
1) Subjects with significant tinnitus who do not “need” hearing aids benefit from a wearable device containing fractal tones and noise alone;
2) Control group subjects receiving only instructional counseling do not show any significant changes in tinnitus distress;
3) Additional components (beyond Zen sound therapy and instructional counseling) of an integrated approach to tinnitus management (WZT) are beneficial, but they need to be individualized;
4) The long-term effects of this treatment extend out to at least 12 months.
The results from this and previous clinical studies strongly support the use of Zen alone, and of the integrated Widex Zen Therapy approach in tinnitus patient management. This individualized, comprehensive approach combining counseling (instructional and adjustment-based cognitive behavioral intervention), amplification, fractal tones and/or noise, and relaxation strategies, is highly effective in reducing tinnitus handicap in a short period of time. The longer-term efficacy of this treatment may be dependent on continued use of the device. Given the high prevalence of hearing loss (often too mild to clearly warrant the need for hearing aids), the benefit of having a tinnitus device that can be reprogrammed with amplification is an added value.
References
-
Shekhawat GS, Searchfield GD, Stinear CM. Role of hearing aids in tinnitus intervention: a scoping review. J Am Acad Audiol. 2013;24:747-762.
-
Trotter MI, Donaldson I. Hearing aids and tinnitus therapy: a 25-year experience. J Laryngol Otol. 2008;122:1052-1056.
-
Folmer RL, Carroll JR. Long-term effectiveness of earlevel devices for tinnitus. Otolaryngol Head Neck Surg. 2006;134:132-137.
-
Surr RK, Montgomery AA, Mueller HG. Effect of amplification on tinnitus among new hearing aid users. Ear Hear.1985;6:71-75.
-
Melin L, Scott B, Lindberg P, Lyttkens L. Hearing aids and tinnitus—an experimental group study. Br J Audiol. 1987;21:91-97.
-
Tunkel D, Bauer C, Sun G, Rosenfeld R, Chandrasekhar S, Cunningham ER, Archer S, Blakley B, Carter J, Granieri E, Henry J, Hollingsworth D, Khan F, Mitchell S, Monfared A, Newman C, Omole F, Phillips C, Robinson S, Taw M, Tyler R, Waguespack R, Whamond E. Clinical practice guideline: Tinnitus. Otolaryngol Head Neck Surg. 2014; 151 (Suppl 2):S1-S40.
-
Reavis K, Rothholtz V, Tang Q, Carroll J, Dhalilian H, Feng FG. Temporary suppression of tinnitus by modulated sounds. J Assoc Res Otolaryngology (JARO). 2012, 13(4): 561-571.
-
Sweetow R. The use of fractal tones in tinnitus patient management. Noise and Health. 2013; 15:63; 96-100.
-
Liikkanen L. Inducing involuntary musical imagery: An experimental study. Musicae Scientiae. 2012. 16 (2): 217–234
-
Hann D, Searchfield G, Sanders M, Wise K. Strategies for the selection of music in the short-term management of mild tinnitus. Australian New Zealand J Aud. 2008:30:129-140.
-
Kuk F, Peeters H, Lau CL. The efficacy of fractal music employed in hearing aids for tinnitus management. Hearing Review. 2010; 17(10):32-42. Available at: https://hearingreview.com/2010/09/the-efficacy-of-fractal-music-employed-in-hearing-aids-for-tinnitus-management
-
Sweetow, R & Sabes, J. H. Effects of Acoustic stimuli delivered through hearing aids on tinnitus. J Am Acad Audiol, 2010. 21, 461-473.
-
Herzfeld M, Kuk F. A clinician’s experience with using fractal music for tinnitus management. Hearing Review. 2011; 18(11): 50-55. Available at: https://hearingreview.com/2011/10/a-clinicians-experience-with-using-fractal-music-for-tinnitus-management
-
Henry J, Wilson P. The Psychological Management of Chronic Tinnitus. Boston: Allyn Bacon;2001.
-
Sweetow, R. Cognitive Aspects of Tinnitus Patient Management: Ear and Hearing. 1986. 7( 6): 390-396.
-
Sweetow, RW, Jeppesen, AMK. A new integrated program for tinnitus patient management. Widex Zen Therapy. Hearing Review. 2012. 19(7), 20-26. Available at: https://hearingreview.com/2012/07/a-new-integrated-program-for-tinnitus-patient-management-widex-zen-therapy
-
Andresson G, Valdo V. Cognitive Behavioral Therapy with applied relaxation. In: Tyler RS, ed. Tinnitus Treatment: Clinical Protocols. New York: Thieme; 2006:176-186.
-
Meikle MB, Henry JA, Griest SE, Stewart BJ, Abrams HB, McArdle R, Myers PJ, Newman CW, Sandridge S, Turk DC, Folmer RL, Frederick EJ, House JW, Jacobson GP, Kinney SE, Martin WH, Nagler SM, Reich GE, Searchfield G, Sweetow R, Vernon JA. (2011) The Tinnitus Functional Index: Development of a New Clinical Measure for Chronic, Intrusive Tinnitus. Ear Hear.32 (5), 1-24.
-
Newman CW, Jacobson GP, Spitzer JB. Development of the Tinnitus Handicap Inventory. Archives of Otolaryngology—Head and Neck Surgery, 1996; 122, 143–148.
-
Davis PB, Wilde RA, Steed LG, Hanley PJ. Treatment of tinnitus with a customized acoustic neural stimulus: a controlled clinical study. Ear, Nose, Throat Journal 2008. 87:330-339.
-
Henry JA, Schechter MA, Nagler SM, Fausti SA. Comparison of tinnitus masking and tinnitus retraining therapy. J Am Acad Audiol. 2002; 13(10):559-81.
-
Herzfeld M, Ciurlia-Guy E, Sweetow R. Clinical trial on the effectiveness of Widex Zen Therapy. Hearing Review. 2014. 22(11). Available at: https://hearingreview.com/2014/10/clinical-trial-effectiveness-widex-zen-therapy-tinnitus
-
Sweetow R, Fehl M, Ramos P. Do Tinnitus patients continue to use amplification and sound therapy post habituation? Hearing Review. 2015; 21(11); 24-29; 201422(3); 34-39. Available at: https://hearingreview.com/2015/02/tinnitus-patients-continue-use-amplification-sound-therapy-post-habilitation
-
Mackenna L, Irwin R. Sound Therapy for tinnitus–sacred cow or idol worship?: an investigation of the evidence. Audiolol Med. 2008; 6.16-24.
Robert Sweetow, PhD, is professor of otolaryngology and former director of audiology at the University of California, San Francisco (UCSF); Francis Kuk, PhD, is executive director at the Widex Office of Research in Clinical Amplification (ORCA-USA), Lisle, Ill; and Sueli Caporali, PhD, was a research audiologist at Widex A/S, Lynge, Denmark.
Disclosure: Dr Sweetow is a part-time paid consultant for Widex A/S, and Dr Kuk is an employee of Widex A/S.
Correspondence can be addressed to HR or Dr Sweetow at: [email protected]
Original citation for this article: Sweetow R, Kuk F, Caporali S. A controlled study on the effectiveness of fractal tones on subjects with minimal need for amplification. Hearing Review. 2015;22(9):30.




It’s nearly impossible to find well-informed people about this topic, but you sound like you know what you’re talking about! Thanks Mitchell