A new patient-driven fitting tool called SoundPoint provides the patient with a means for fine-tuning a hearing aid by moving a pointer on a computer display or Apple iPad™ screen. Movement of the pointer to different areas of the screen results in instantaneous changes to the frequency shaping, gain, and compression parameters of the hearing aid.
As discussed in an article by Abrams et al1 in last month’s edition of The Hearing Review, several established prescriptive fitting algorithms exist to precalculate gain and compression settings based on audiometric data. These approaches are designed to provide an average fitting for a particular audiogram, but cannot account for the individual’s unique loudness growth or loudness discomfort level.
It is not surprising then that new fitting algorithms from Australia’s National Acoustic Laboratories (NAL), Cambridge University (Camfit), and the University of Western Ontario (DSL) prescribe significantly different first-fit parameters for an individual hearing loss. Regardless of the fitting algorithm—or selected fitting philosophy—a perfect match to target is unlikely to be perceived as “perfect” by an individual patient. Instead, it is likely that adjustments from this starting place will be required to arrive at acceptable sound quality settings for the individual.

Susie Valentine, PhD, and J. Andrew Dundas, PhD, are research audiologists, and Kelly Fitz, PhD, is a senior DSP research engineer at Starkey Laboratories Inc, Eden Prairie, Minn. Correspondence can be addressed to HR or Dr Valentine at .
Translating abstract patient comments into appropriate programming changes is one of the most challenging aspects of fitting hearing aids. Patients may have difficulty clearly articulating their auditory experience. Clinicians may be faced with several different, yet equally viable fine-tuning approaches to addressing these comments and are therefore forced to follow a question-and-answer approach. We refer to this interaction as an “interview and adjust” approach to fine-tuning hearing aids.
In an effort to ease and improve the patient fitting experience, a patient-driven fitting system named SoundPoint was developed to provide patients intuitive control of the hearing aid fitting process while attempting to preserve the audibility of the speech signal.1 SoundPoint provides the patient with a means for seamless fine-tuning of the hearing aid by simply moving a pointer on a computer display or Apple iPad™ screen. Movement of the pointer to different areas of the screen results in instantaneous changes to the frequency shaping, gain, and compression parameters of the hearing aid.
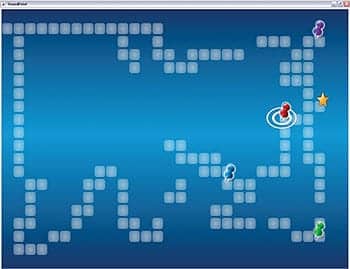
FIGURE 1. Screenshot of a patient’s navigation through the SoundPoint environment. Areas visited are highlighted by a trail of blocks. Points of interest are indicated by colored pushpins. Favorite settings are indicated by a star.
When the SoundPoint system is activated in Starkey’s Inspire 2011™ software, the hearing aids are connected automatically via wireless or wired link, and the calibration process is initiated. A speech-shaped calibration noise is played from a desktop loudspeaker, and the microphones of the hearing aids are used as the reference microphones to calibrate the level of the signal. Once the presentation level of the stimulus has been calibrated, a specially prepared speech-in-noise stimulus developed from the Connected Speech Test (CST)2 is presented in a background of multi-talker babble at a level approximating that of average speech. The patient is greeted by a set of on-screen directions inviting them to explore the SoundPoint environment shown in Figure 1.
As the patient explores the SoundPoint screen, sound quality changes smoothly in real time. When the patient finds a point in the screen with a desirable sound quality, they indicate favorites by clicking (or tapping if the optional iPad interface is used). A click of the mouse or tap on the screen places a small pushpin icon, marking the location as having desirable sound quality settings. After the patient has identified several preferred points, they can easily compare settings and indicate an overall favorite. The settings judged to be optimal are programmed into the hearing aid when SoundPoint is closed.
The SoundPoint system can be used with any of the prescriptive fitting algorithms supported by Inspire 2011™, or the patient can fine-tune existing settings that are stored in their hearing aid to optimize sound quality.
Clinical Validation of System
The purpose of this study was to compare participant reactions and the quality of fittings obtained via traditional audiologic methods (wherein adjustments were made by an experienced clinician in response to patient report) to those obtained with the SoundPoint fitting system.
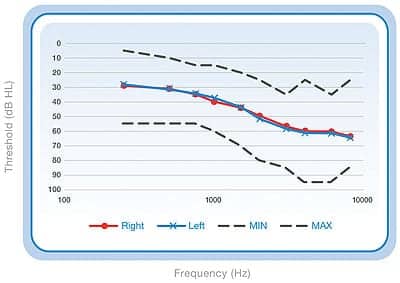
FIGURE 2. Mean audiometric thresholds for 29 participants, circles represent the right ear and Xs represent the left ear. Dashed lines represent the maximum and minimum hearing threshold.
Subjects and hearing aid fittings. A total of 29 listeners (17 males, 12 females) participated in this study, and their mean age was 71 years old (range of 56 to 82 years). All participants had mild to moderately severe symmetric sensorineural hearing loss (Figure 2). The majority of participants (25) were experienced hearing aid users.
During the study, participants wore Starkey S-Series iQ 11 behind-the-ear (BTE) hearing aids with appropriately vented custom earmolds, and completed two 2-week field trials. Field Trial 1 was completed with the clinician fitting, while Field Trial 2 was completed with the SoundPoint fitting. Audibility of both fittings was verified via probe microphone measurements conducted with an Audioscan Verifit probe microphone system, and fitting/field trial order was randomized and counterbalanced.
Field Trial 3 was a 1-week trial that allowed multi-memory comparisons of both fittings. At the conclusion of the field trials, participants performed blinded paired comparison testing to identify the preferred fitting with respect to sound quality and perceived speech intelligibility.
The SoundPoint fitting environment was populated with the participants’ best-fit parameters according to e-STAT (Starkey’s proprietary fitting formula) and 10 predetermined parameter sets (presets) that would permit a limited range of frequency shaping, gain, and compression adjustments from the initial e-STAT fitting. The presets were arranged to allow smooth, perceptually intuitive changes in sound quality as the individual moved the mouse pointer around the screen. Changes to gain and compression could be applied in different combinations across the frequency range of the hearing aid in order to change the perceptual experience in different ways. Four different but equivalent preset layouts were generated so that we could assess the ability of the participants to select similar hearing aid settings on repeated navigations.
For this initial investigation, participants navigated through the SoundPoint fitting environment while listening to a recording of a male voice. The speech stimulus was presented in quiet (14 participants) or mixed with a background of cafeteria babble background noise (15 participants) at +10 dBSNR. Both stimuli were presented from a single loudspeaker at 0° azimuth. While moving the mouse pointer, participants listened to the changing settings in the hearing aids, and selected their preferred settings. This process was repeated with each of the four layouts, and the participant then chose their favorite selection after comparing the favorite selected in each of the four navigations. Real ear aided response (REAR) measures were obtained at soft, average, and loud speech input levels using an Audioscan Verifit probe microphone system. At the conclusion of each fitting session, participants completed a survey to evaluate the current fitting; a second Web-based survey was also completed in order to evaluate the usability of SoundPoint.
During Field Trials 1 and 2, participants were instructed to seek out five specified listening environments typically identified as challenging by listeners with hearing impairment, and to volunteer additional listening situations of personal concern. For each listening situation, participants completed a modified version of the Glasgow Hearing Aid Benefit Profile (GHABP).3
Field Trial 3 allowed the participants to blindly compare the clinician and SoundPoint fittings by toggling between two hearing aid programs. Participants used a written diary to estimate the relative loudness of the environment and indicate a program preference for the five specified listening environments from the previous field trials and environments of concern. Blinded paired comparison testing was used to assess participant program preference in terms of sound quality and subjective speech intelligibility.
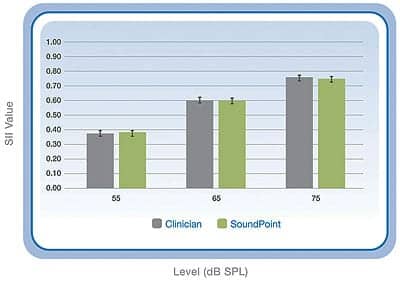
FIGURE 3. Mean SII and standard error for n=29 hearing impaired participants. SII values are shown for soft (55dB), average (65dB), and loud (75dB) speech inputs.
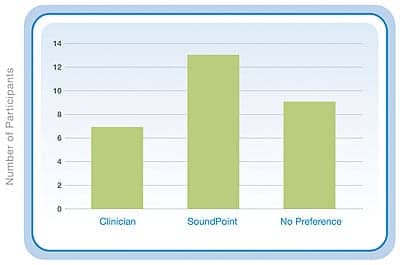
FIGURE 4. Overall preference ratings from the field trial for each of fitting approaches.
Results
The individual fittings were assessed from objective and subjective perspectives as described above. These evaluations included quantitative measures of audibility, prediction of speech intelligibility performance on CST sentences,4 subjective assessment of sound quality, perceived speech understanding via paired comparison testing, and subjective preference in the field.
Speech Intelligibility Index5 values for soft, average, and loud input were calculated from real-ear measurement data obtained with both SoundPoint and clinician fittings. Figure 3 shows the mean SII values obtained at soft, average, and loud input levels for both fittings. No significant differences in calculated audibility were observed between fitting procedures, suggesting that use of the patient centered fitting system would provide similar audibility to the clinician fitting for the three speech level inputs tested.
No significant differences in calculated audibility were observed between navigations performed while listening to speech in quiet versus speech in noise; however, it was observed that, while using SoundPoint, participants who listened to speech in noise were able to navigate to more consistent hearing aid settings on the four alternative layout navigations. Based on patient report, it was hypothesized that the addition of background noise to the speech stimulus made it easier to identify preferred fitting settings than when listening to speech in quiet.
Speech Intelligibility Index values were next used to calculate predicted performance on the CST using the transfer function described by Sherbecoe and Studebaker.4 As expected, predicted performance increased with stimulus presentation level, and no significant differences were observed between fitting conditions. This indicates that participants were able to navigate to preferred settings that should produce similar speech intelligibility performance to that obtained via traditional fitting methods.
Fitting preference was investigated in a blinded all-pairs comparison test in which each fitting was compared to each of the others a total of 10 times. Participants listened to the stimulus that they had used to perform the fitting navigation during these trials. One set of comparisons was performed to investigate preference in terms of perceived sound quality, while a second set was performed to investigate preference in terms of perceived speech intelligibility.
TABLE 1. Preference for each of the fitting techniques. Values represent the number of participants wherein a statistically significant preference was observed for one fitting technique over another. Preferences were established for 1) sound quality, and 2) perceived speech intelligibility. The leftmost column of boxes represents a set of comparisons and the following two columns list the number of statistically significant preferences for the fitting approaches.
Table 1 summarizes the paired-comparison test results for the 29 participants. The numbers listed illustrate the number of participants who had statistically significant preferences for the specific comparison. Participants preferred the sound quality obtained via the SoundPoint fitting over the clinician fitting and an unaltered e-STAT “best fit” based on the audiogram. In terms of subjective speech understanding, participants selected the SoundPoint fitting as superior 4 times more often than the clinician fitting, and also more frequently than the e-STAT fitting.
During the Field Trial 3, participants were asked to blindly compare the clinician settings and SoundPoint settings in the field via multi-memory switching. Figure 4 shows preference for each of the fitting approaches. SoundPoint settings were preferred by more participants than the clinician settings (13 versus 7); while 9 participants indicated that they either had no preference between the two settings or were unable to hear a difference between them. Despite the fact that 7 participants preferred the clinician fitting, and 9 did not indicate a preference, 27 participants verbally reported that they would be happy to use their SoundPoint settings in the field for an extended period of time.
The usability of SoundPoint was evaluated on four main metrics: 1) ease of use; 2) likability; 3) usefulness; and 4) “learnability.” Figure 5 shows that 90% of participants found that SoundPoint was easy to use, and that 75% of participants would want to use the system to adjust their hearing aids in the future. There were no major learnability issues found with SoundPoint (90% of participants), and 100% of the participants found SoundPoint to be a useful tool for evaluating the sound quality of different fitting parameters. Encouraging results were found for each of these metrics listed above, indicating that—from the patient’s perspective—SoundPoint is a viable clinical tool.
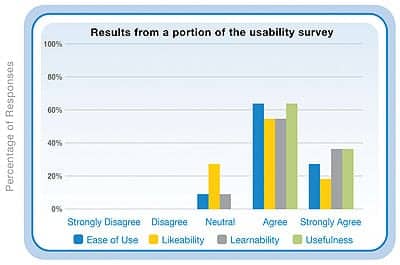
FIGURE 5. Results from selected questions from the usability survey administered to the subjects regarding SoundPoint. Ease of Use is based on the subject response to the statement “I thought that the system was easy to use”; Likeability, the statement “On my next visit, I would want my hearing-aid adjusted using this system”; Learnability, the statement “It was easy to get started when it came to learning how to use the interface”; and Usefulness, the statement “I found the system’s interface (exploring the space with a mouse) an easy way of evaluating the quality of sound settings in my hearing-aid.”
Based on the results of this multi-week field trial, listeners with mild-to-moderate sensorineural hearing losses significantly preferred fittings conducted using the SoundPoint fitting system when compared to either traditional clinician or “best-fit” fitting methods. This observation held true regardless of whether the stimulus used for fitting comparisons consisted of speech in quiet or speech in noise. Fittings conducted with speech in noise, however, resulted in more consistent navigations to sets of fitting parameters that sounded similar.
Audibility and predicted speech intelligibility performance were observed to be similar between the SoundPoint and traditional fittings, suggesting that patients do not sacrifice performance in search of listening comfort. The successful outcome of this study supported the decision to implement the SoundPoint fitting system into Starkey’s products and Inspire fitting software.
Conclusion
SoundPoint provides a number of unique features and opportunities for patients and dispensing professionals alike. It can be used in both initial fittings and follow-ups, and provides the clinician with information regarding desirable fitting settings by allowing real-time monitoring of gain and compression values selected by the patient.
Additional significant benefits lie in the fact that the patient does not need to articulate a complaint to the hearing care professional, and that the professional does not have to interpret that complaint in order to arrive at an acceptable change for that patient. Instead, patients can simply tune the hearing aids to arrive at settings that alleviate their concern.
The SoundPoint system resulted in fittings with similar speech audibility and predicted performance to those fittings generated through a traditional “interview and adjust” fitting. When combined with the observed patient preference for this approach to fitting, and high subjective satisfaction with the fittings attained, SoundPoint should be considered a viable fitting tool.
SoundPoint has been developed to increase patient satisfaction with hearing aids by creating a unique and rewarding partnership between the patient and practitioner.
This paper describes the implementation and validation of an interactive, patient-centered hearing aid fitting tool called SoundPoint. The system provides patients and dispensers with a tool to ease the fine-tuning phase of the hearing aid fitting. SoundPoint is designed to improve patient satisfaction through patient empowerment or “ownership” of the fitting process by creating a unique and rewarding partnership between the patient and practitioner.6
References
- Abrams H, Edwards B, Valentine S, Fitz K. A patient-adjusted fine-tuning approach for optimizing the hearing aid response. Hearing Review. 2011;18(3):18-27.
- Cox RM, Alexander GC, Gilmore C. Development of the Connected Speech Test (CST). Ear Hear. 1987;8(5 Suppl):119S-126S.
- Gatehouse S. Glasgow Hearing Aid Benefit Profile: Derivation and validation of a client-centered outcome measure for hearing-aid services. J Am Acad Audiol. 1999;10:80-103.
- Sherbecoe RL, Studebaker GA. Audibility-index functions for the connected speech test. Ear Hear. 2002;23:385-398.
- American National Standards Institute (ANSI). ANSI S3.5-1997—American National Standard Methods for the calculation of the speech intelligibility index. New York: ANSI; 1997.
- Roberts KJ. Patient empowerment in the United States: a critical commentary. Health Expectations. 1999;2(2):82-92.
Citation for this article:
Valentine S, Dundas JA, Fitz K. Evidence for the use of a new patient-centered fitting tool. Hearing Review. 2011;18(4):28-34.



