A review of noise-reduction strategies, as well as when and how to use them
It’s a noisy world, and noise continues to be a major issue for hearing aid users. This article presents an overview of noise management strategies, general guidelines for assessing patients’ hearing abilities in noise, the intended applications for the various noise reduction strategies, as well as when and how to implement them.
Let’s face it, our environment is noisy. Noise is the second main complaint of all participating consumers when eating at restaurants, according to the Zagat survey.1 Individuals cannot even escape from the noise in their own homes, as noise is the number-one neighborhood complaint.2 Since normal-hearing people are subjected to considerable amounts of noise on a daily basis, it is not surprising that the number-one complaint of all hearing aid users is difficulty hearing in noise; almost half (49%) of those who return their hearing aids reportedly do so because of problems with background noise.3

Rena Appleby, AuD, is an audiologist at the GN ReSound Global Audiology Center in Glenview, Ill.
Normal-hearing people also encounter difficulty hearing in noise, but are better able to capitalize on the redundancies in speech than those with hearing impairment. However, as the background noise, reverberation, or distance is increased, and/or unfamiliar topics are introduced, the natural redundancy of speech decreases.4
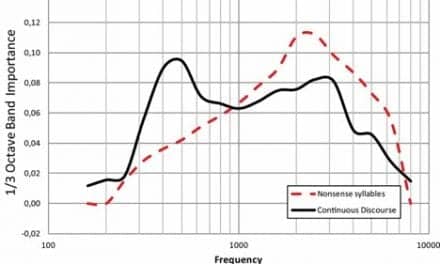
The redundancies in speech are often lost when someone has hearing loss, in part due to certain phonemes or parts of phonemes that might not be audible.5 Auditory coding (frequency resolution) also might not be as precise, which can result in stimulation of additional frequency areas within the cochlea, making it more difficult to differentiate among the sounds being heard. A third problem for those with hearing impairment is the ability to detect changes in the duration of sounds (temporal gap discrimination).5
Older adults with hearing impairment often face other difficulties in addition to the aforementioned problems. Given the same hearing loss configuration, studies have shown that older adults perform worse on speech recognition measures in quiet than younger adults.6 In addition, older adults might experience more difficulty processing language in the presence of competing speech due to cognitive involvement.7
With all of these factors that can contribute to hearing in noise problems, what approach are most clinicians taking and is there more that could be done? According to a Hearing Review dispenser survey,8 most clinicians are using audiograms and speech discrimination measures in quiet on a routine basis as assessment tools for their hearing aid clients. The survey further indicates that less than half of the hearing instrument specialists were routinely performing some type of speech in noise test, although hearing in noise has consistently been the number-one complaint from hearing aids users for years.
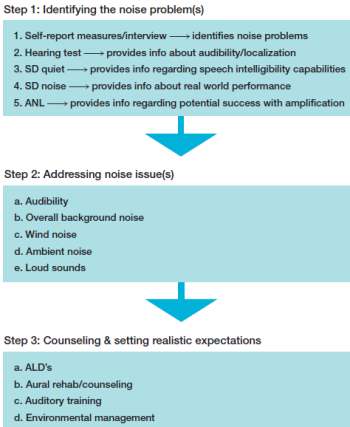
The steps to successful noise management for hearing aids will be reviewed in this article, and an outline of the steps can be found in Figure 1.
Identifying the Source of the Hearing in Noise Problem
Although audibility can easily be predicted from an audiogram, speech recognition ability in quiet is a poor predictor of speech recognition ability in noise.9 Furthermore, significant differences have been reported in the ability to understand speech in noise among hearing-impaired listeners with similar audiograms. Killion et al10 found that pure-tone averages for a group of listeners ranged from 40 to 60 dB, but resulted in SNR scores that were either comparable to those of normal-hearing listeners or comparable to those with a severe loss of ability to hear in noise.
In order to address the hearing in noise complaints, it is important to measure hearing in the various auditory domains that can contribute to hearing in noise difficulties.9 In general, there are three domains for assessing these difficulties:
- Basic auditory function or the audiogram;
- Speech discrimination ability in quiet;
- Speech discrimination ability in noise.
Speech-in-noise tests. Most clinicians are familiar with the typical tests used for assessing function of the first two auditory domains. There are many different tests that can be used for assessing the third auditory domain, speech discrimination ability in noise. The HINT11 and the QuickSIN12 are two tests that can provide clinicians with information regarding the patient’s signal-to-noise ratio (SNR) needs. Sentences are presented at different SNRs using speech babble noise. Both tests provide normative data so that the patient can be compared to their normal-hearing peers. The HINT provides scores in a threshold format whereas the QuickSIN provides data in a SNR loss format. The QuickSIN also provides a chart that offers amplification recommendations for patients who present with different SNR losses.
ANL and validation measures. In addition to assessing the auditory domains, there are two other measures that can be invaluable when working with a patient complaining of difficulty hearing in noise. The Acceptable Noise Level (ANL) test can be administered in 2 to 3 minutes pre/post hearing aid fitting and is reportedly 85% accurate at determining whether a given patient will be a successful hearing aid user.11 Success is directly equated with an individual’s ability to tolerate background noise, with successful hearing aid users having a higher tolerance of noise or lower ANL score. Successful users are considered to be those with ANL scores below 7 dB, while unsuccessful users are those with ANL scores above 13 dB.
Studies conducted at the University of Tennessee have shown that ANL scores can be improved when digital noise reduction (DNR) and/or directional microphones are utilized.13 Results show the biggest improvement in ANL scores (8 dB) was seen when directionality and DNR were used in combination. Hearing aid users further expressed a preference for both, although each one reportedly resulted in an average ANL improvement of 4 dB. More studies are needed to determine if these findings translate outside the clinic environment. 13Interviewing and self-report measures provide information about the patient’s experiences that cannot be obtained from any other measures. These can include open-ended tests, such as the COSI or GHABP, which allow patients to individualize responses, or can be close-ended multiple-choice tests, such as the APHAB, HASS, or HHIE, which allow results to be compared to normative data.14 There are advantages and disadvantages to both. Open-ended measures are customized for each individual and enable the patient to elaborate on problems they are having. However, due to the customized nature of the questionnaire, results cannot be compared to normative data. Close-ended measures easily allow for comparison of the patient’s responses to their hearing-impaired peers, but some of the questions may not be relevant and/or might not address all of the issues the person is having. Information from the questionnaires can show which environments the patient is finding the most problematic, as well as provide information regarding whether the patient is encountering more difficulty than his/her hearing-impaired peers.
Addressing Noise Issue(s)
Auditory or central nervous system dysfunction can result in hearing in noise complaints, as can hearing aids that are considered to be a good fit or those that are not a good fit. The results from the self-report measure, audiogram, speech discrimination measures, and the ANL test should assist the clinician in determining the contributing factors to the noise problem(s).
Audibility. Current American Academy of Audiology (AAA) guidelines recommend performing real-ear measurements (REM) as a tool for verifying hearing aid gain in adult patients.15 REM can be used to provide objective information regarding whether incorrect gain is a contributing factor in reported hearing in noise problems.
The gain values that the manufacturer recommends for a given hearing aid user in the fitting software assume the patient has an average-size ear canal. Therefore, if a given patient has a larger-than-average ear canal, they may not receive enough gain and could complain that speech is not loud enough or that noise is too loud due to a primary audibility issue. Likewise, if the patient has a smaller-than-average ear, the hearing aids may provide too much gain, resulting in everything being too loud, including noise.
In addition, audibility—especially in noise—can generally be improved by fitting hearing-impaired patients with two hearing aids instead of only one, when possible. According to Kochkin, “Such benefits include better hearing in quiet and noise, better sound quality, better localization of sounds, and higher listening comfort in various situations.”16
Although some studies have shown an improvement in the ability to understand speech in noise when fit binaurally, there may not be an improvement in the actual acceptance of noise.17 Studies also have shown there is a small segment of the elderly population who may actually perform better on speech recognition in noise tests when fit monaurally due to possible binaural interference.18
Overall background noise. If your patient is complaining about the overall level of background noise, the problem could be due to noise that is mixed in with the signal of interest or noise that is being amplified in other areas along with the signal of interest.
Noise that is embedded in the signal of interest. It is extremely difficult to develop a hearing aid algorithm that removes all of the noise embedded in speech without eliminating or distorting a portion of the desired speech signal. Studies have shown the primary benefit of noise reduction to be improved listening comfort, with essentially no improvement in speech understanding.19,20 Most hearing aids on the market today have a noise reduction algorithm that uses modulation rate/depth or spectral subtraction to eliminate unwanted noise from the signal. Modulation-based noise reduction systems “use modulation rates to identify the presence or absence of speech and use modulation depth to estimate the SNR in the incoming signal,”21 with the amount of gain reduction that occurs dependent on the manufacturer’s algorithm and the noise reduction settings in the software.
Spectral subtraction reduces noise by consistently monitoring the gaps between the speech sounds in order to generate an accurate noise spectrum. The noise spectrum is then subtracted from the speech signal, with the amount of gain reduction dependent on the manufacturer’s algorithm and the noise reduction settings within the software.
Enabling noise reduction or increasing the noise reduction gain for the environment(s) in which the patient is experiencing difficulty hearing in noise can be especially helpful in improving listening comfort.
Noise that is separated from the signal of interest. Directional processing can be helpful when a patient complains that he/she is having difficulty hearing in noise, and the speaker or signal of interest is separated out from the unwanted noise. Directional microphones are the most effective noise reduction strategy in hearing aids, and are reported to provide a 3 to 4 dBSNR improvement in real-world environments with low reverberation.21,22
There are several basic directional technology schemes that can be selected for a given hearing aid user. Fixed directionality is best at cancelling noise located behind the hearing aid user when the speaker or signal of interest is located in front of the user.
Adaptive directional processing can be helpful when a hearing aid user is confronted with multiple noise sources. With adaptive directionality, multiple noise sources in different locations can be cancelled out at the same time.
Some manufacturers also offer directional programs that automatically change beamwidth based on the SNR in the environment or allow users to change the beamwidth using a remote control device to enable them to better focus in on the signal of interest. In addition, several manufacturers offer wireless ear-to-ear capability, which allows for synchronization of the directional microphones for both ears and has been shown in studies to result in an overall improvement in speech understanding.
There are several different ways in which hearing aid users can access the directional programs within their hearing aids. Users can change the programs manually by using a button located on the hearing aids or by using a remote control device. If a hearing aid user is not capable of manually switching the programs or is not interested in doing so, most hearing aids on the market offer automatic switching programs. Automatic switching programs constantly monitor the SNR in the environment and change the processing strategy to an omnidirectional mode when the SNR is more favorable and change to a directional processing strategy when the SNR is less favorable. Automatic switching programs are helpful in that hearing aid users do not have to manually change back and forth between programs.
However, the drawback to their use is that the automatic switching programs make assumptions regarding the preferred processing for a particular environment and might not actually be in agreement with the actual preferences of the hearing aid user. In order to circumvent this problem, one manufacturer advocates using asymmetric microphone fittings in which the worse ear is fit with omnidirectional processing and the better ear is fit with fixed directionality. With this configuration, the hearing aid user is able to retain environmental awareness, while at the same time benefit from a reduction in background noise, with speech understanding in noise comparable to dual microphone fittings.23
Wind noise. “Wind noise generated by random turbulent flow across the hearing aid microphone(s) can be a mere annoyance or a debilitating interference for hearing aid users,” according to a 2010 study by Chung.21 Research has shown that wind noise interference can vary based on the style of hearing aid, the processing being used, and the direction of the wind flow.21,24
As a general rule, the best way to reduce the annoyance of wind noise is to prevent it from entering the hearing instrument in the first place. Some custom device styles, such as CICs that fit deeper into the ear or remote microphone instruments in which the placement of the microphone lies within the contours of the ear, offer natural wind noise protection. Other hearing aid styles, such as BTEs, are more susceptible to wind noise.
Microphone mode is also important. According to Thompson, “With a directional microphone, the interfering wind noise that is generated very close to the microphone is sensed with high sensitivity while the desired sound from the far field is sensed with low sensitivity. Whenever there is a choice, the directional microphone on a hearing aid should not be used when wind noise is present.”25 Thus, fitting a patient with a single microphone hearing instrument or utilizing a program with omnidirectional processing can reduce wind noise complaints.
In addition to the above options, many manufacturers offer software-based wind noise programs that are designed to reduce gain in the frequencies in which wind noise is detected. Possible issues with such wind noise reduction features are that they may detect wind noise when it is not actually present, or they may fail to detect wind noise when it is. The result can be annoying gain reductions at unwanted times, or lack of comfort in windy conditions.
Ambient noise. Although wide-dynamic range compression (WDRC) and/or directionality can be quite beneficial, they also can create a problem: ambient noise.
“WDRC is used to restore audibility for weak sounds and simultaneously restore some of the normal loudness perception that is lost with recruitment,” according to Killion.26 In order to accomplish this, more gain is applied to low-level input sounds than high-level input sounds, with “input signal levels below the threshold of compression typically receiving linear amplification,” writes Plyler.27
Expansion was designed to reduce the ambient noise caused by WDRC. Expansion works in the opposite way that compression does in that less gain is applied to very soft sounds being picked up by the microphone. To address ambient noise complaints due to WDRC, clinicians can try enabling or increasing the amount of expansion set within the fitting software, when possible. If this is not possible or does not work, reducing the gain for soft low-frequency sounds might be of benefit.
Traditional directional processing is not as sensitive to low frequency sounds, which has resulted in manufacturers using bass boost to address the problem. With bass boost, additional gain is applied to low frequency sounds, which can result in low frequency environmental noise and hearing aid microphone noise being over-amplified. This problem can often be addressed by turning off the bass boost or by reducing the amount of bass boost that is being applied. In addition, several manufacturers offer split-band directionality, which processes low frequencies in an omnidirectional manner and high frequencies in a directional manner, thus preserving the low frequency information. Because bass boost is not needed when using split-band directionality, ambient noise is not typically an issue with this type of processing.
Loud sounds. If loud noises are intolerable, but all other sounds are okay, it is likely that the patient’s UCLs for at least some of the frequencies have been exceeded. Real-ear and coupler verifications of loud sounds are excellent ways to verify that loud sounds are tolerable to the patient. Measured results can be compared to the patient’s actual or predicted UCLs to adjust hearing aid gain and output.
Counseling and Setting Realistic Expectations
The main goals when fitting amplification are to improve audibility and to increase the signal-to-noise ratio, resulting in an overall improvement in speech understanding. Even with amplification, some patients will still encounter significant hearing problems due to a damaged auditory system, reduced cognitive ability, and/or difficult auditory environment.
Therefore, it is important to use the subjective and objective test results to counsel the patient about realistic expectations. If the patient demonstrates a significant SNR loss, he/she might benefit from assistive listening devices (ALDs), aural rehabilitation/counseling, or computer-based auditory training programs in addition to amplification.
With all of the wireless hearing aids in the market today, many new ALDs have been introduced that can improve the SNR by offering direct connectivity to TVs, phones, iPods, or remote microphones.
In addition, studies have shown that, when hearing aid users attend group support programs, on average they have fewer return visits and report their hearing aids to be beneficial in more listening environments than those who do not attend a group.28,29 Computer-based auditory programs also can be helpful in improving speech understanding ability in noise.30 The Seeing and Hearing program31 provides online training in lip reading, while the LACE program32 provides online training for understanding speech in noisy environments.
While technology and training can help improve the SNR for hearing-impaired people, noise will always be an issue that even normal-hearing people have to contend with on a daily basis. The best option continues to be starting out with a good SNR by being selective about the environment when possible, and manipulating the environment when necessary.
Clinicians can be most beneficial to their hearing-impaired patients by providing them with hearing tools—not just hearing aids—and these tools should include ALDs, counseling, and listening strategies.
Correspondence can be addressed to Dr Appleby at .
References
- Zagat survey. Available at: www.restaurantmagazine.com/tag/zagat/. Accessed April 2, 2012.
- American Housing Survey (2009). Available at: www.census.gov/housing/ahs/data/national.html
- Kochkin S. MarkeTrak VIII: New opportunities for promoting hearing solutions. Available at: www.betterhearing.org
- Palmer C. Amplification and the impact on cognitive demand. 2010. Available at: www.entsociety.co.za/Congress/09h30_Palmer_Cognitive_Demand_Wedn.pdf
- Ross M. Hearing in noise. SHHH Journal. March/April 1996. Available at: Hearingresearch.org/ross/hearing_loss/hearing_in_noise.php
- Kricos P. Audiologic management of older adults with hearing loss and compromised cognitive/psychoacoustic auditory processing capabilities. Trends Amplif. 2006;10(1):1-28.
- Tun P, O’Kane G, Wingfield A. Distraction by competing speech in young and older adult listeners. Psychol Aging. 2002;17:453-467.
- Strom K. The HR 2006 dispenser survey. Hearing Review. 2006;13(6):16-39.
- McArdle R, Wilson R. Selecting speech tests to measure auditory function, 2008. Available at: www.asha.org
- Killion MC, Niquette PA, Gundmundsen GI, Revit LJ, Banerjee S. Development of a quick speech-in-noise test for measuring signal-to-noise ratio loss in normal-hearing and hearing-impaired listeners. J Acoust Soc Am. 2004;116:2395-2405.
- Nilsson M, Gelnett D, Sullivan J, Soli S, Goldberg R. Norms for the Hearing In Noise Test: The influence of spatial separation, hearing loss, and English language experience on speech reception thresholds. J Acoust Soc Am. 1992:94(4, pt 2):2291-2385.
- Niquette P, Gudmundsen G, Killion M. QuickSIN Speech-in-Noise Test Version 1.3. Elk Grove Village, Ill: Etymotic Research; 2001. Available at: www.etymotic.com/pro/quicksin.aspx
- Plyler P. Acceptance of background noise: recent developments. Hearing Journal. 2009;62(4):10,12,14-17.
- Taylor B. Self-report assessment of hearing aid outcome—an overview; 2007. Available at: www.audiologyonline.com/articles/article_detail.asp?article_id=1888
- American Academy of Audiology. Guidelines for the Audiology Management of Adult Hearing Impairment; 2008. Available at: www.audiology.org
- Kochkin S. Binaural hearing aids: the fitting of choice for bilateral loss subjects. PDF available at: www.betterhearing.org/pdfs/Binaural_hearing_aid_complete_review.pdf
- Freyaldenhoven M, Plyler P, Thelin J, Burchfield S. Acceptance of noise with monaural and binaural amplification. J Am Acad Audiol. 2006;17(9):659-66.
- Blay A. Critical Review: Do elderly hearing aid users perform better on speech recognition in noise tests when fitted monaurally or binaurally? 2010. PDF available at: publish.uwo.ca/~larchiba/2010%20pdfs/Blay.pdf
- Mueller G, Weber J, Hornsby B. The effects of digital noise reduction on the acceptance of background noise. Trends Amplif. 2006;10:283-293.
- Bentler R, Wu Y-H, Kettel J, Hurtig R. Digital noise reduction: outcomes from field and lab studies. Int J Audiol. 2008;47(8):447-460.
- Chung K. Reducing noise interference: strategies to enhance hearing aid performance. ASHA Leader. 2010;15(4):10-13.
- Ricketts T. Directional hearing aids. Trends Amplif. 2001;5(4):139–176.
- Bentler R, Egge J, Tubbs J, Dittberner A, Flamme G. Quantification of directional benefit across different polar response patterns. J Am Acad Audiol. 2004;15:649-659.
- Stender T, Hielscher M. Windguard: bringing listening comfort to windy conditions. 2011. Available at: www.gnresound.com
- Thompson S. Directional microphone patterns: they also have disadvantages. 2000. Available at: www.audiologyonline.com/articles/article_detail.asp?article_id=219
- Killion MC. Compression: Distinctions. Hearing Review. 1996;3:29-32.
- Plyler P. Applying expansion in hearing aid fittings: subjective and objective findings. 2007. Available at: www.audiologyonline.com/articles/article_detail.asp?article_id=1885
- Kricos P. Group support programs for new hearing aid users. 2003. Available at: www.audiologyonline.com/articles/article_detail.asp?article_id=42129
- Brickley GJ, Cleaver VCG, Bailey S. An evaluation of a group follow-up scheme for new NHS hearing aid users. Brit J Audiol. 1996;30:307-312.
- Kricos P. Tips for hearing in noise: Part III. 2008. Available at: www.betterhearing.org/aural_education_and_counseling/articles_tip_sheets_and_guides/tips_for_hearing_in_noise.cfm
- Bauman N. Seeing and Hearing Speech Program. Available at: www.hearinglosshelp.com/products/seeinghearingspeech.htm
- Sweetow R. Physical therapy for the ears: maximizing patient benefit using a listening retraining program. Hearing Review. 2005;12(10):56-58.
Citation for this article:
Appleby R. Noise Management in Modern Hearing Aid Fittings Hearing Review. 2012;19(05):44-51.