“Whattage” represents the frequency with which a listener uses “What?”, cognate words, or behaviors that prompt repetitions by a communicatively significant other. The concept of “Whattage” has broad implications for marketing the value of hearing correction to the general public, as well as individual members of the communicative dyad.
Patient Care | June 2017 Hearing Review
A toolkit for getting the patient and significant others to start practicing better hearing
Within the market-critical demographic of adults 50 years and older with self-admitted impairments of refractive vision or peripheral hearing, there is a sharp contrast between the 90% reported acceptance of vision correction1,2 and a 30% acceptance of hearing aids.3,4
There exists a palpable cognitive dissonance between contemporary reports of a 75-85% hearing aid user satisfaction rating5,6 and a 70% outright rejection of corrective amplification. Among the non-accepting hearing-impaired, most reject the concept of corrective amplification entirely, while a minority—somewhere around 4.7%7 to 24%8—reject hearing aid(s) after a perceived negative experience.
The key reasons for the a priori rejection of hearing aids from two well-known authors9,10 are presented in Table 1. In both lists, denial of need for hearing help transcends perceived excessive cost as a demotivating factor.

Table 1. Reasons why people do not seek hearing help, as demonstrated by Kochkin and Trychin.
Traditionally, the cost of hearing aids—Kochkin’s reason #39 and Trychin’s reason #410 in Table 1—has been cited as the primary deterrent to acceptance of corrective amplification. Most recently, reports from the 2015 President’s Council of Advisors on Science and Technology (PCAST)11 and National Academies of Science, Engineering, and Medicine (NASEM),12 indict excessive cost as the primary barrier to hearing aid use. Both organizations postulate a solution by legitimizing a less costly, over-the-counter (OTC) class of essentially self-fitted corrective amplification.
Some statistics on hearing aid use in other countries provide a wider aperture on the issue (Figure 1).14-16 Based on these data, 58% of Norwegians and Swiss with self-identified hearing impairment decline to use hearing aids—even if the cost is heavily (75%-100%) subsidized!
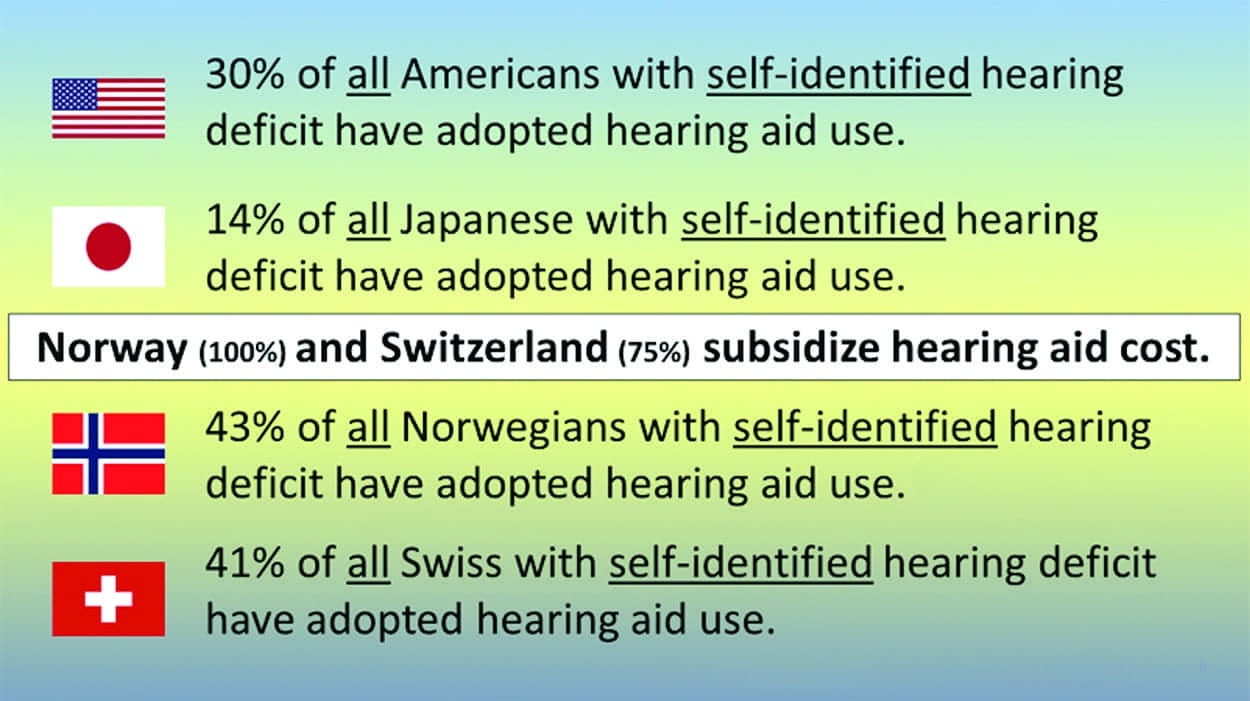
Figure 1. Comparisons of hearing aid use by those with self-identified hearing loss, as reported by MarkeTrak 9 and EuroTrak (2015).
Other than cost, what factor(s) can demotivate more than two-thirds of the US senior population with self-admitted hearing impairment from considering hearing aid use? The answer is implicit in the top-two reasons for a priori rejection of hearing aids provided by both Kochkin9 and Trychin10 (Table 1)—lack of awareness of hearing impairment or partial/full denial of the need for hearing correction.
It is helpful to draw a contrast between acceptance of vision and hearing correction.
Impaired Vision vs Impaired Hearing
There are a number of basic elements common to the successful, non-medical remediation of both (refractive) vision and (peripheral) hearing impairment.
1) A clinically verified loss of acuity relative to accepted norms (ie, a measured sensory impairment);
2) A context in which the loss of acuity attains functional significance, essentially defining disability;
3) Self-awareness of the impairment, the disability, or both, and
4) Self-acceptance of an appropriately fitted form of correction.
This categorization is consistent with the 2003 World Health Organization (WHO) revision of the International Classification of Functioning, Disability, and Health17 and dovetails with the biopsychosocial model of health and disability conceptualization as summarized in Falvo.18 Further, this contrasts with a traditional medical model that bases a diagnosis of impairment on test outcomes, such as the Snellen chart for visual acuity and the pure-tone audiogram for hearing acuity.
With regard to hearing rehabilitation outcomes, the medical model relies on real ear measurement verification that a nominal pure-tone, audiogram-based hearing aid fitting criterion has been achieved. Alternatively, the biopsychosocial model would rely upon a pragmatic assessment of fitting success, using such behavioral instruments as the Hearing Handicap Inventory for the Elderly (HHIE)19 or an anecdotal determination of improvement provided by the patient and communicatively significant other(s) (CSO). While not eschewing the scientific basis for assessment and non-medical remediation of hearing loss, there should be professional latitude for the concept of Behavioral Audiology. Figure 2 compares some basic functions potentially impacted by vision and hearing impairment.
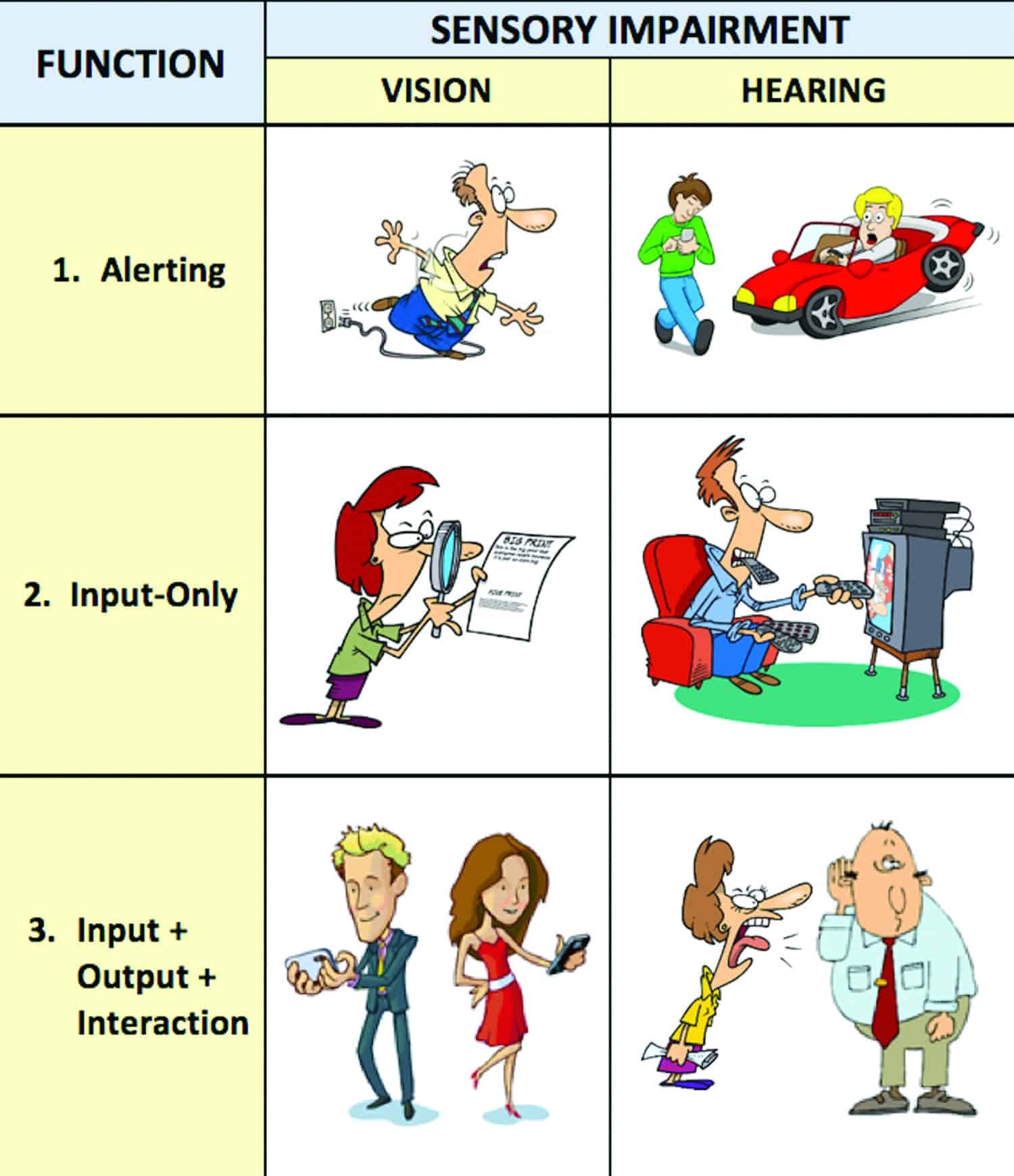
Figure 2. Three categories of function impacted by vision and hearing impairment.
1) Alerting. Both senses provide a basic alerting function for safety and survival that may be affected, proportional to the degree of impairment.
2) Input-only. A common element of the input-only category is the impaired perception of non-interactive textual content in lexical or acoustic format. The only option available in the visual example is enhancement of text through use of optical correction. In the TV example, the listener modifies the acoustic signal directly by increasing its amplitude or by supplementing it visually with superimposed closed captioning.
3) Input + Output + Interaction. A crucial inter-sensory divergence occurs when the informational transfer paradigm is bi-directional. Other than smartphone texting, there is no functional visual parallel to an interactive oral-aural interchange. The unaided hearing-impaired listener sends cues to the talker or CSO, indicating misperception and the need for more information. The CSO responds to the prompt, reflexively repeating, restating, and attempting to repair the original flawed communicative interchange. (As detailed below, the listener’s aggregate cueing behavior can be termed “Whattage.”)
The relative success of the listener’s behavior mitigates a self-perceived hearing disability at the expense of the CSO’s effort. The favorable outcome for the listener facilitates denial of any significant impairment and effectively lessens motivation to consider the alternative of personal corrective amplification. In this context, the CSO functions as an inadvertent enabler of listener denial.
The critical nature of the CSO is reflected in a quotation from Helen Keller’s 1910 correspondence with physician James Kerr Love:
“I am just as deaf as I am blind. The problems of deafness are deeper and more complex, if not more important, than those of blindness. Deafness is a much worse misfortune. For it means the loss of the most vital stimulus— the sound of the voice that brings language, sets thought astir, and keeps us in the intellectual company of man.”20
This quotation, concerning the relative personal impact of deafness and blindness, templates the communicative dyad as a critical context in which the various manifest degrees of hearing acuity loss become a unique sensory handicap. Conversely, reduced or absent interaction with the CSOs essentially limits the opportunity for handicap to be defined functionally. The CSO category may include spouses, children, grandchildren, friends, and caring co-workers. In contrast, vision impairment exists more-or-less independently of interpersonal interaction.
“Whattage”
There are numerous grammatical forms of the one-word utterance: “What.” The specifically targeted form of “What?”, including its cognates, corresponds to “I heard you but I didn’t hear you clearly enough to understand fully what you said. Please repeat” (Figure 3). The listener sends a cue to the talker in a communicative dyad that the spoken message content has not been received accurately, prompting repetition, increased emphasis, or rephrasing from the talker. A comparable transaction is created when the listener articulates misperceived content back to the talker, often creating a mondegreen21 (eg, “going to choir practice” misheard for “going to the chiropractor’s”).22 In the context of conversational analysis,23 “Whattage” prompts a transaction of informational interchange called a repair.
Figure 3. The many forms of “Whattage.”
As shown in Table 2, the content-clarification-eliciting form of “Whattage” can be generated by conditions existing in the talker (T), the environment (E), or the listener (L). A total of 7 of the 8 listed sources of “Whattage” in Table 2 do not include peripheral, sensory hearing impairment. Consequently, in the course of any normal conversational interchange, some baseline level of “Whattage” can be expected. The addition of a high frequency or other form of hearing loss, with sufficient residual hearing to stimulate auditory awareness of incoming conversation, increases the “Whattage.”

Table 2. Conditions that prompt listeners to ask “What?”, as well as the sources for confusion (T = Talker; E = Environment; and L = Listener).
Noteworthy as a source of “Whattage” is an adult manifestation of Auditory Processing Dysfunction (APD). The reported incidence of APD in children ranges between 2-3%.24 The condition is known to persist through adulthood with incidence estimated at 5%,25 excluding traumatic brain injury. The combination of hearing impairment and APD presents a high degree of challenge to a successful hearing instrument fitting.
Similarly, there has been considerable research recently into what has collectively become known as “hidden hearing loss.” Some of these studies have demonstrated that, while cochlear function (and pure-tone hearing loss relative to the audiogram) can resolve after initial onset of temporary threshold shift (TTS), there can still be inner hair cell (afferent) synaptic loss, rapid inner hair cell dendritic loss, spiral ganglion cell loss, and persistent reductions in suprathreshold neural responses (ie, reduced wave I ABR).26-29 Likewise, Barbara Timmer30 and others have written about how the consequences of “mild hearing loss” for some people is not “mild” in terms of their auditory perception and abilities.
The author, in his busy practice, sees an average of one to two middle-aged patients a month, predominantly female, referred by primary care physicians (PCPs) with the chief complaint of hearing difficulty in noise, presenting with no measurable loss of hearing acuity at the time of visit. The combination of APD or “hidden hearing loss” with hearing impairment is especially challenging for remediation via hearing aids.
In the speculative “Whattage” repair function (Figure 4), asymptote of repairs is reached when the magnitude of loss exceeds the listener’s awareness of loud speech (65 dB HL) or when the talker’s patience fails. From a biopsychosocial perspective, the goal of a hearing aid fitting is to minimize “Whattage” and restore accuracy to a conversational interchange, lessening the need for repairs by the CSO. Functionally, the degree of post-fitting “Whattage” should be reduced sufficiently to satisfy both parties in the communicative dyad.
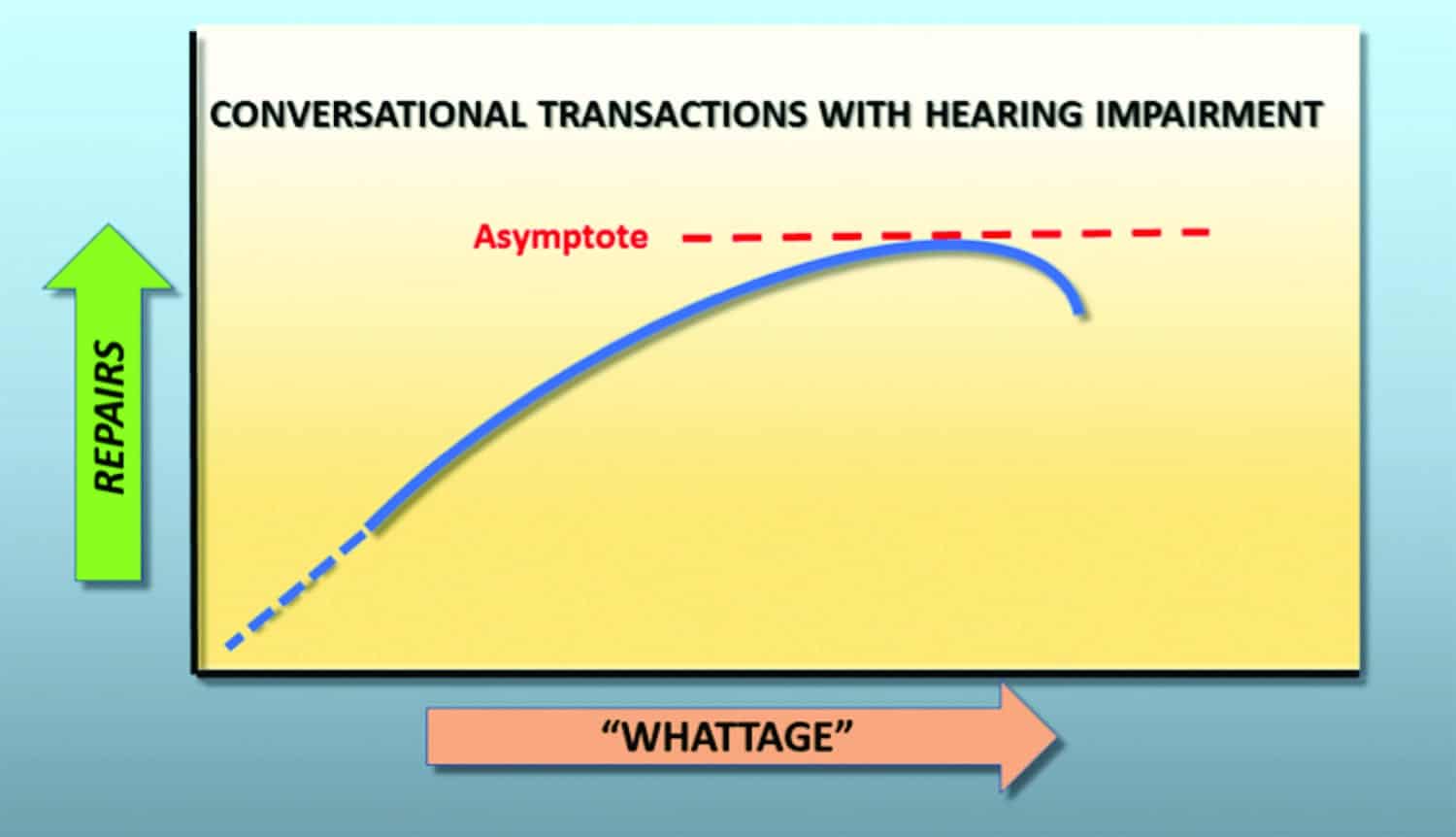
Figure 4. The “Whattage” repair function in which the asymptote is reached when the magnitude of “whattage” or misunderstanding due to hearing loss exceeds the listener’s awareness of loud speech or when the talker’s patience fails him/her.
Gender Differences and “Whattage”
Where loss of hearing impacts the accuracy of a received conversational transaction, the listener frequently denies responsibility while cuing the talker who reflexively makes content repairs. Gender differences also play a significant part in this process. Women are more likely to respond to “Whattage” cues from both women and men. As Tannen31 states:
“For most women, the language of conversation is primarily a language of rapport: a way of establishing connections and negotiating relationships…For most men, talk is primarily a means to preserve independence and negotiate and maintain status in a hierarchical social order.”31
Table 3 summarizes some of Tannen’s observations31 on gender differences in communicative style. In a spousal relationship, wives tend to experience a continuity of communicative connectivity (rapport) with their husbands. Husbands tend to connect communicatively with their wives on demand (report). Contrary to spousal intuition, husbands are not always tuned to “Channel Wife”—a prime source of “Whattage.” In striving for connectedness, women, in turn, are more responsive to “Whattage” prompts from both men and women. Table 4 summarizes some gender differences in attitudes toward hearing impairment according to Garstecki and Erler.32-34

Table 3. Some of Tannen’s observations on gender differences in communicative style.
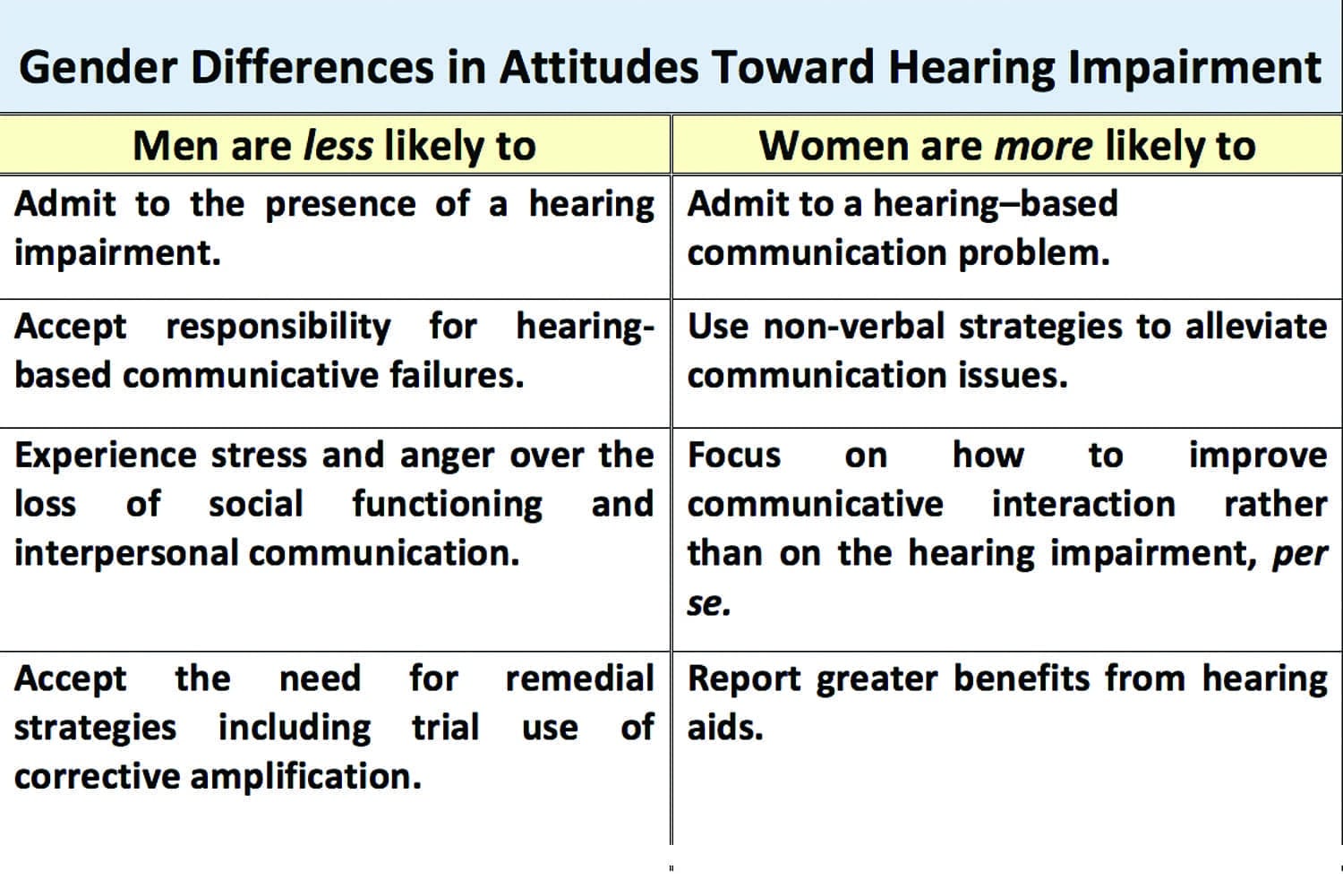
Table 4. Some gender differences in attitudes toward hearing impairment.
“Whattage”: Implications for Consumer Education
The “Whattage” construct facilitates for both parties in the communicative dyad—listener and talker/CSO—a better understanding of their respective roles in the impaired conversational transaction. The role of the CSO as an enabler of denial can be further modeled and studied; the dependency role of the hearing-impaired listener can be demonstrated and quantified. There would appear to be value in enlightening both members of the communicative dyad, rather than targeting one or the other.
Most advertising in the hearing industry is directed either to the hearing aid candidate or to the caring other. Given the interactive nature of “Whattage,” it is suggested that an advertising/informational campaign—at the government public service or corporate level—should focus on the concept of unaided hearing impairment as a burden shared and perpetuated by both listener and talker.
“Whattage” may be introduced in public service presentations by hearing professionals on the topic of hearing loss and its non-medical treatment. Attendees at these events are generally dissatisfied hearing aid users who are looking for solutions. A typical audience is comprised of unaided individuals, aware to some degree of their own hearing limitations, aided individuals dissatisfied with aided outcomes, CSOs, or both members of the communicative dyad, typically in a spousal, dependent, or close familial relationship (mother/daughter, father/son, grandchildren, etc).
The “Whattage” Kit
The author has devised a technique for heightening awareness of “Whattage.” The “Whattage” Kit includes a “Whattage” Hearing Self-Check (Figure 5), as well as instructions for the Whattage” Self-Assessment (Figure 6), cardstock “Whattage” tokens (top right of Figure 6, also available in a 1-page sheet in the online version of this article), and “Whattage”-reduction recommendations for the CSO (Figure 7).
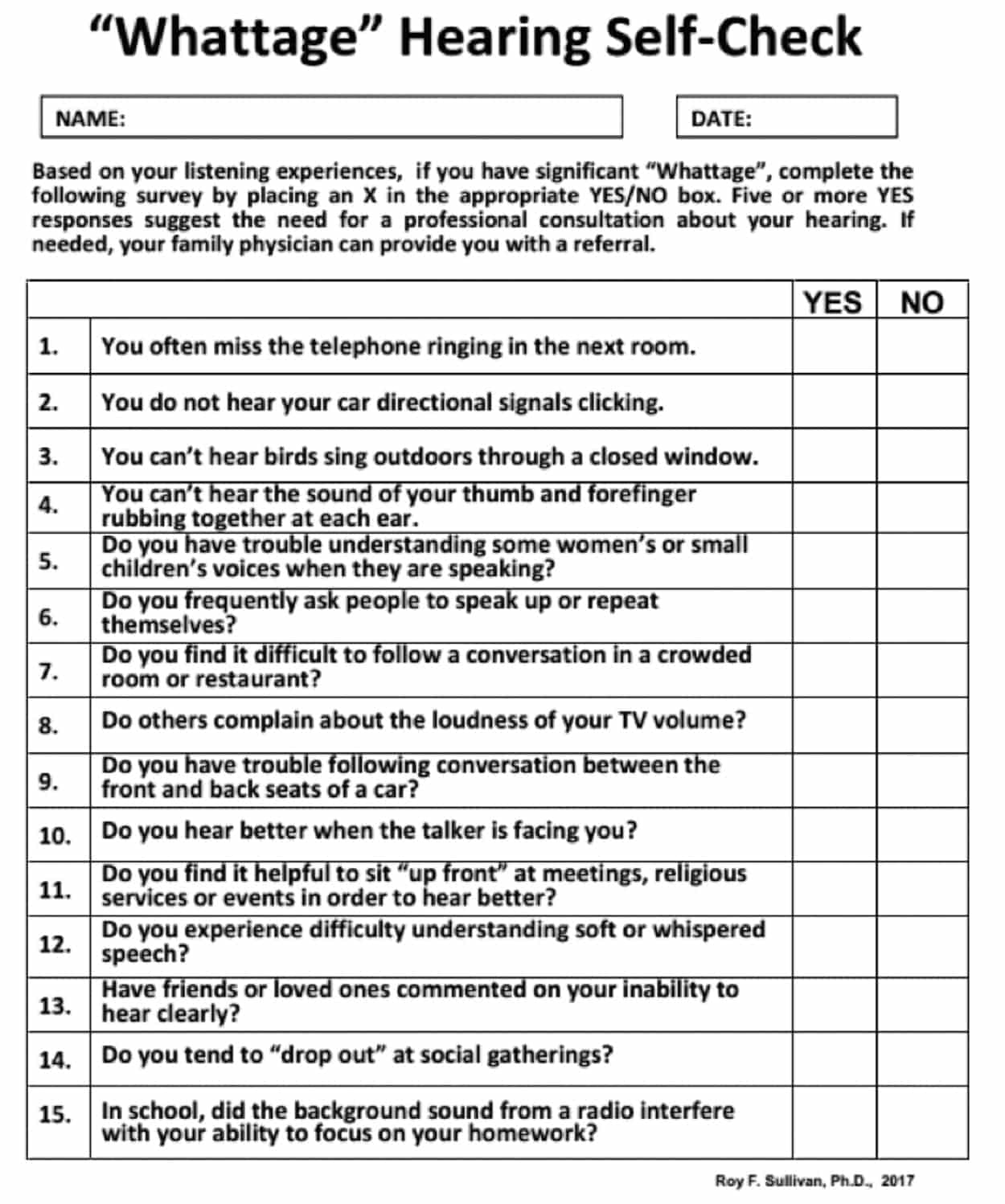
Figure 5. “Whattage” Hearing Self-Check.

Figure 6. The “Whattage” Self-Assessment Kit.

Figure 7. The “Whattage”-reduction recommendations for the communicatively significant other (CSO).
In the “Whattage” Hearing Self-Check (Figure 5), Items 1-5 and 12 relate to high frequency hearing; Items 6, 8, 10, and 13 reference the CSO; Items 7, 9, and 15 concern noise impact; and Items 11 and 14 concern modification of listener behaviors. Item 15 might also relate to adult APD or hidden hearing loss. While this test is not a “validated” checklist, it can be used as a helpful measure for gauging “Whattage.” In this example, 5 or more “YES” responses suggest the need for further action; the patient is encouraged to consult with a hearing care professional or Primary Care Physician (PCP) and/or referral to a known audiological resource. This can also be helpful in alerting the local PCP community of your professional availability. (A customizable version of each component in the “Whattage Kit” is available in the online version of this article.)
In a dispensing practice, “Whattage” can be introduced at number of different stages. For example, when a CSO calls on behalf of a potential patient, a “Whattage” Kit is included in the mailed introductory materials. It can be introduced as a construct in the initial clinical interview where the new patient, accompanied by a CSO, is reluctant to admit to a hearing impairment. The “Whattage” kit assessment process is most likely to be implemented by the CSO.
For an unaccompanied reluctant patient, the concept is explained and a “lower my ‘Whattage” cue card (Figure 7) is offered with instruction to share it with his/her CSO. In doing so, the listener effectively acknowledges the need for hearing support and the talker’s role in the conversational repair process is validated. The cue card is also of value when, for varying reasons, an optimized hearing instrument fitting provides significant but sub-optimal reduction in “Whattage.” In the author’s practice, the cue card is included with each dispensing.
When both talker and listener are “on the same page,” the likelihood increases for the acceptance of corrective amplification as an alternative to misunderstanding and stress in the communicative dyad.
Summary
A number of variables mitigate personal awareness of a hearing impairment and reduce motivation to pursue corrective amplification. “Whattage” is a hypothetical construct that represents the frequency with which a listener uses “What?”, cognate words or behaviors to prompt repetitions by a communicatively significant other (CSO.) There are no such parallel communicative interactions inhibiting access to vision correction. Gender differences in communicative style enhance compliance. The concept of “Whattage” has broad implications for marketing the value of hearing correction to the general public as well as individual members of the communicative dyad. ?
Acknowledgements
The author gratefully acknowledges the review and suggestions provided by Michael Valente, PhD, and Allan Mehr, DA.
References
- Densai M, Pratt L, Lentzner H, Robinson K. Trends in vision and hearing among older Americans. Aging Trends. 2001;(2)[Mar]:1-8. Available at: https://www.ncbi.nlm.nih.gov/labs/articles/11894223/
-
Newport F. Forty percent of Americans who use glasses would consider laser eye surgery. March 6, 2000. Available at: http://www.gallup.com/poll/3115/forty-percent-americans-who-use-glasses-would-consider-laser-eye-surgery.aspx
-
Abrams HB, Kihm J. An introduction to MarkeTrak IX: a new baseline for the hearing aid market. Hearing Review. 2015;22(6)[Jun]:16-21. Available at: https://hearingreview.com/2015/05/introduction-marketrak-ix-new-baseline-hearing-aid-market
-
National Institutes on Deafness and Other Communication Disorders (NIDCD). Quick statistics about hearing. December 16, 2015. Available at: https://www.nidcd.nih.gov/health/statistics/quick-statistics-hearing
-
Kochkin S, Beck DL, Christensen LA, et al. MarkeTrak VIII: The impact of the hearing healthcare professional on hearing aid user success. Hearing Review. 2010;17(4):12-34. Available at: https://hearingreview.com/2010/04/marketrak-viii-the-impact-of-the-hearing-healthcare-professional-on-hearing-aid-user-success
-
Calderone J. Hearing loss: No more suffering in silence. February 2, 2017. Consumer Reports. 2017; March:15-20. Available at: http://www.consumerreports.org/hearing-aids/hearing-loss-no-more-suffering-in-silence
-
Hougaard S, Ruf S. EuroTrak I: A consumer survey about hearing aids. Hearing Review. 2011;18(2)[Feb]:12-28. Available at: https://hearingreview.com/2011/10/eurotrak
-
Hartley D, Rochtchina E, Newall P, Golding M, Mitchell P. Use of hearing aids and assistive listening devices in an older Australian population. J Am Acad Audiol. 2010 Nov-Dec;21(10):642-53. doi:10.3766/jaaa.21.10.4.
-
Kochkin S. MarkeTrak VII: Obstacles to adult non-user adoption of hearing aids. Hear Jour. 2007;60(4)[Apr].
-
Trychin S. Why don’t people who need them get hearing aids? 2003. Available at:http://users.clas.ufl.edu/mcolburn/Web-links/Nursing%20Lecture/Why%20Don%27t%20People%20Who%20Need%20Them%20Get%20Hearing%20Aids.htm
-
President’s Council of Advisors on Science and Technology (PCAST). Aging America & Hearing Loss: Imperative of Improved Hearing Technologies [letter report to President Obama]. October 26, 2015. Available at: https://obamawhitehouse.archives.gov/sites/default/files/microsites/ostp/PCAST/PCAST%20hearing%20letter%20report.pdf
-
National Academies of Sciences, Engineering, and Medicine. Hearing Health Care for Adults: Priorities for Improving Access and Affordability. Washington, DC: The National Academies Press; 2016. Available at: https://www.nap.edu/catalog/23446/hearing-health-care-for-adults-priorities-for-improving-access-and
-
Abrams HA, Kihm J. An introduction to MarkeTrak IX: a new baseline for the hearing aid market. Hearing Review. 2015;22(6):16-21. https://hearingreview.com/2015/05/introduction-marketrak-ix-new-baseline-hearing-aid-market/
-
European Hearing Instrument Manufacturers Association (EHIMA). JapanTrak 2015. Zurich, Switzerland: Anovum. Available at: http://www.ehima.com/wp-content/uploads/2016/02/JAPAN_Trak_2015-1.pdf
-
European Hearing Instrument Manufacturers Association (EHIMA). Eurotrak Norway 2012, Switzerland. Zurich, Switzerland: Anovum. Available at: http://www.ehima.com/wp-content/uploads/2014/03/protected_eurotrak_2012_norway.pdf
-
European Hearing Instrument Manufacturers Association (EHIMA). Eurotrak Switzerland 2015. Zurich, Switzerland: Anovum. Available at: http://www.ehima.com/wp-content/uploads/2016/02/EuroTrak_2015_SWITZERLAND_final.pdf
-
US Centers for Disease Control and Prevention (CDC). The ICF: An overview. Available at: https://www.cdc.gov/nchs/data/icd/icfoverview_finalforwho10sept.pdf
-
Falvo D. Medical and Psychosocial Aspects of Chronic Illness and Disability. 5th Ed. Bartlett, Mass: Jones and Bartlett;2014.
-
Ventry IM, Weinstein BE. The Hearing Handicap Inventory for the Elderly: A new tool. Ear Hear. 1982;3(3):128-134.
-
Love JK. The deaf child from the viewpoint of the physician and teacher. Laryngoscope. 1920;20:596.
-
Wright S. The death of Lady Mondegreen. Harper’s Magazine. 1954;Nov.
-
Sacks O. Mishearings. New York Times. June 5, 2015. Available at: https://www.nytimes.com/2015/06/07/opinion/oliver-sacks-mishearings.html
-
Schegloff EA, Jefferson G, Sacks H. The preference for self-correction in the organization of repair in conversation. Language. 1977;53(2):361-382.
-
Chermak G, Musiek F. Central Auditory Processing Disorders: New Perspectives. San Diego: Singular Publishing;1997.
-
Saunders G, Haggard M. The clinical assessment of obscure auditory dysfunction–1. Auditory and psychological factors. Ear Hear. 1989;10(3):200-208.
-
Salvi R, Sun W, Ding D, et al. Inner hair cell loss disrupts hearing and cochlear function leading to sensory deprivation and enhanced central auditory gain. Frontiers Neurosci. 2017; 10:[Jan 18]:621. doi:10.3389/fnins.2016.00621
-
Kujawa SG, Liberman MC. Acceleration of age-related hearing loss by early noise exposure: Evidence of a misspent youth. J Neurosci. 2006; 26(7):2115–2123.
-
Kujawa SG, Liberman MC. Adding insult to injury: Cochlear nerve degeneration after “temporary” noise-induced hearing loss. J Neurosci. 2009; 29(45):14077-14085.
-
Maison SF, Liberman MC. Predicting vulnerability to acoustic injury with a noninvasive assay of olivocochlear reflex strength. J Neurosci. 2000;20:4701-4707
-
Timmer B. It may be mild, slight, or minimal, but it’s not insignificant. Hearing Review. 2014;21(4):30-33. Available at: https://hearingreview.com/2014/04/may-mild-slight-minimal-insignificant
-
Tannen D. You Just Don’t Understand! Women and Men in Conversation. New York City:HarperCollins;1990.
-
Garstecki D, Erler S. Hearing loss, control, and demographic factors influencing hearing aid use among older adults. J Speech Lang Hear Res. 41(3):527-37, 1998
-
Garstecki D, Erler S. Older adult performance on the Communication Profile for the Hearing Impaired: Gender difference. J Sp Lang Hear Res. 1999;42:785-796.
-
Garstecki D, Erler S. Hearing loss–and hearing aid–related stigma: Perceptions of women with age-normal hearing. Am J Audiol. 2002;11(2)[Dec]:83-91.
Correspondence can be addressed to HR or Dr Sullivan at: [email protected]
Original citation for this article: Sullivan RF. “Whattage”: A hypothetical construct in hearing healthcare. Hearing Review. 2017;24(6):20-28.




I have seen this in my practice.
This reference may be helpful:
https://www.ncbi.nlm.nih.gov/pubmed/21812630
Nice job. I’m wondering if you know whether chemotherapy can cause the speech-recognition score to drop, with no change in pure-tone thressholds?
A high resolution .pdf of the “WHATTAGE” toolkit for customized use is available at this link:
http://gchs-sullivan.com/attachments/File/WHATTAGE_KIT_REPRINTa.pdf